|
|
Short Communication Indian Pediatrics 2007; 44:838-841 |
|||||||||||||||||||||||||||||||
|
Cefpodoxime Proxetil Compared with Cefixime for Treatment of Typhoid Fever in Children |
|||||||||||||||||||||||||||||||
|
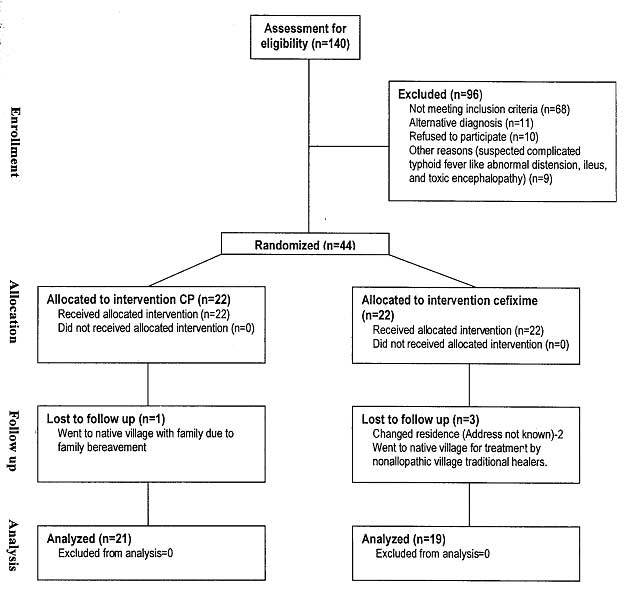
Emergence of multidrug resistant (MDR) typhoid fever in the late 1980s, in many parts of the world including Indian subcontinent, prompted to evaluate new agents particularly orally active antibiotic for the treatment of typhoid fever(1-4). There are published reports that cefixime (CF) a third generation cephalosporin is effective in treating typhoid fever and well practiced in typhoid fever(5-7). Cefpodoxime Proxetil (CP) is widely used in pediatric infectious diseases except typhoid fever; it is almost similar to cefixime in its pharmacological and antimicrobial properties(8) but cheaper than cefixime. Till date there are no published controlled studies evaluating CP in invasive typhoidal salmonellosis. We, therefore, undertook a pilot study where we prospectively evaluated the clinical and bacteriological efficacy of oral CP therapy for children suffering from culture confirmed typhoid fever and compared with that of oral cefixime with the hypothesis that CP is effective in treating typhoid fever. Subjects and Methods During a 16 months period (March 2003 to June 2004), children between 6 months to 12 years with clinical features suspected of typhoid fever were assessed for eligibility. Patients taking antibiotics for preceding 72 hours and suspected complicated typhoid fever like abdominal distension, ileus, toxic encephalopathy was excluded. Study flow chart is provided in Fig. 1.
In all provisionally selected children blood was drawn for complete blood count, widal and blood culture. However, only culture confirmed typhoid fever were finally enrolled for RCT. Children were enrolled in the study after taking written informed consent from their parents and prior approval of ethical review committee of the hospital. A repeat blood culture was done on 10th day of therapy or on earlier date in case of unsatisfactory clinical response. All isolates were tested for susceptibility and minimal inhibitory concentrations (MIC) of the antibiotics were determined. Eligible children were allotted to double blind RCT to receive either oral CP (16 mg/kg/day divided every 12 hours, Group-A) or CF (20 mg/kg/day divided every 12 hours, Group-B). Simple randomization technique was done using a computer program. Medicines were supplied in bottles that were similar in size, shape and colour and without any commercial label. The bottles were coded and only the principal investigator who was not directly involved in delivering drugs to patients knew which bottle contained which drug. Neither the patient nor the attending physician, appointed to the study knew which of the two drugs the patients received. Patients were followed up on 3rd, 5th, 7th and 10th day of treatment at medical outpatient of the hospital or at home by medical assistant in case of failure to attend at hospital. Clinical defervescence was defined as temperature below 37.5ºC for at least 48 hours without antipyretic. A satisfactory clinical response or clinical effectiveness (clinical cure) was defined as complete resolution of all presenting symptoms and signs after 10 days of therapy. Bacteriological cure was defined as elimination of originally isolated pathogens. At the end of the therapy the cost of the antibiotic actually given to each patient in both groups were calculated according to manufacturer’s suggested retail price. Statistical package for social science (SPSS) software version 11.5 for windows were used for all statistical analysis. Results Of 140 children assessed for suspected typhoid fever, 40 (CP = 21, CF = 19) completed the study. The two group showed similar clinical response with similar defervescence in days (Group-A, 4.87 ± 2.33 d vs Group-B, 4.27 ± 2.28 d, P = 0.308) and similar clinical cure with only one clinical failure in each group who was subsequently treated with ceftriaxone (Table I). Both the children with clinical failure showed bacteriological eradication on subsequent blood culture. The MIC of CP and CF in all Salmonella typhi isolated (n = 40) was <4 µg/mL (range 2-8 µg/mL) and <0.5 µg/mL (range 0.25- 1 µg/mL) respectively. No relationship was found between pretreatment febrile illness in days and clinical cure (r = 0.038, P = 0.707) and no significant relationship was found between nutritional status and days required for defervescence (r = –0.057, P = 0.566). TABLE I Comparison of Baseline Characteristics, Clinical and Bacteriological Response in two Groups
* Results of significance for “defervescence in days” between Cp and Cf (P = 0.308). ** Results of significance for “clinical cure” between CP and CF (P = 0.972). No significant side effects were observed during the course of therapy. In Group-A one child presented with mild maculopapuler rash and in Group-B one child developed mild diarrhea, both of them were self limiting not requiring drug withdrawal. Both Cefixime and Cefpodoxime proxetil were well tolerated by all children. Calculation of cost of an average therapeutic course showed Cefpodoxime proxetil to be cheaper than Cefixime (taka 784/- vs. taka 1040/- equivalent to US$ 12 vs US$ 16 respectively). Discussion Our study revealed comparable efficacy of twice daily oral Cefpodoxime proxetil to oral cefixime in children suffering from typhoid fever. The time of defervescence in our study were found earlier than controlled trial of Bhutta, et al. with cefixime but similar to open study of Girgis, et al.(3,4). No significant side effects were observed in either group during the course of therapy. Diarrhea with CF and CP of mild to moderate intensity were also found to be side effects in western studies(9-11). Cefpodoxime proxetil can be used in children on daily dose from 4 mg/kg/day to more than 16.5 mg/kg/day(12). Fujii R, et al.(13) found no significant side effects or tolerance problem by using Cefpodoxime proxetil in a dose of 20 mg/kg/day in various childhood infections. From the study results we concluded that Cefpodoxime Proxetil is an effective and cheap oral option for treatment of uncomplicated typhoid fever in children. However, it was a pilot study and there-fore further studies with more culture confirmed typhoid patients are needed in order to validate our findings. Contributors: MS was the principal investigator, conceived the idea and provided the study design and drafted the manuscript. SA was the senior pediatrician involved in assessing the case for eligibility and inclusion of case in the study. JS and HM were involved in case selection and case management and follow up. MA provided intellectual input. MS, SA and MA also analyzed and interpreted the results. Funding: Aristopharma Limited. Competing interests: We have received funds for research and for speaking at symposia from Aristopharma Pharmaceutical Company. However we are not members of Aristopharma advisory board.
| |||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||
|
|
![]()