|
|
Research Papers Indian Pediatrics 2007; 44:830-837 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Fluconazole Prophylaxis against Fungal Colonization and Invasive Fungal Infection in Very Low Birth Weight Infants |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
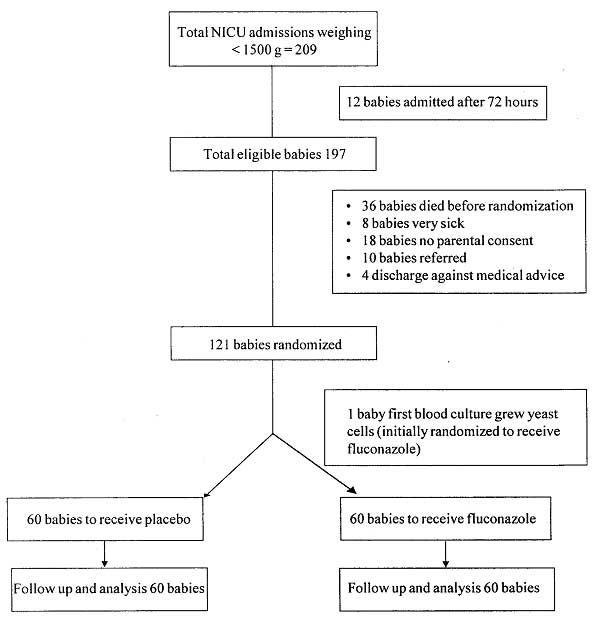
The incidence of systemic fungal infection in newborn has been observed to range from 2.2% to 12.9% among very low birth weight (Birth weight <1500 g) infants and from 5.5% to 16.5% among those <1000 g(1-4). Study from North India demonstrated 22.8% rate of invasive fungal infection in preterm babies staying for more than one week in the Neonatal Intensive Care Unit (NICU)(5). Fungal sepsis in neonate is associated with frequent end organ dissemination (22% to 34%) and high mortality(6). It has been shown that Candida species rapidly colonize the skin and mucous membranes of about 40-60% of critically ill infants and can progress to invasive infection(7,8). Colonization with Candida species is one of the most important predictor of invasive disease(9). Reducing fungal colonization may prevent the development of invasive fungal infection in preterm infant(10). The study was carried out to determine if prophylactic Fluconazole decreases the incidence of Candida colonizations and invasive fungal infection in Very Low Birth Weight (VLBW) infants. Subjects and Methods This prospective, double blind, randomized controlled trial was conducted at our Level III NICU. Study Period was for one year from October 2003 to September 2004. VLBW infants admitted to Neonatal Intensive Care Unit (NICU) within first 72 hours of life were included in the study. Critically ill neonate and neonates with hepatic insufficiency as demonstrated by aspartate aminotransferase (AST) or alanine aminotransferase (ALT) elevation >4 times normal values for gestational age (>244 IU /L or >152 IU IL, respectively) were excluded. Infants with first blood culture (at enrolment) growing Candida sp. were excluded after initial inclusion. Randomization was done at the time of enrolment to receive either solution A or solution B (one of them being Fluconazole and other being placebo) by the shuffled sealed envelope method. Baseline data on the demographic and clinical characteristics of the infants was collected and relevant clinical data was prospectively collected throughout the course of the study on a pre-designed proforma. Presence of one or more clinical signs consistent with fungal infection (e.g., temperature instability, increase in frequency of apnea, increase in oxygen requirement, ashen gray color, etc.) were noted. Fungal surveillance cultures were collected on the day of randomization (day 1 to 3) and days 7, 14, 21, 28 and also as indicated by the treating physician. Surveillance cultures were collected as: rectal swab, oropharyngeal swab, skin swab from groin, umbilical swab (collected only on the day of randomization) and blood for fungal culture by venepuncture. Swabs were obtained using sterile cotton swab. Blood for fungal culture was obtained by venepuncture and collected in brain heart infusion broth; 0.5 mL blood was collected in 5 mL of broth. Solution A or solution B was administered intravenously at a dose of 3mL/kg/day as a single dose every 72 hours till day 7 and subsequently every 24 hours till day 28 of life or till discharge from hospital whichever is earlier. Fluconazole preparation used for the study was colorless, in the strength of 1 mL = 2 mg. The placebo group received an equal volume of normal saline as it physically matched the Fluconazole solution. The drugs were given intravenously till baby reached full feeds and subsequently orally powder form (6 mg/kg) was used. Placebo group received equal amount sugar powder which was physically similar in appearance to Fluconazole powder. Drugs or Placebo were dispensed as Solution A or Solution B from pharmacy. Drug or placebo were administered by a trained senior staff nurse specifically assigned for this work. Aspartate transaminase (AST) and Alanine transaminase (ALT) levels were measured to assess for hepato-toxicity on the day of randomization and on days of life 7, 14, 21 and 28 till the time patients were on solutions. Any medical event not explained by the underlying disease condition of the baby was noted separately and weekly reviewed. The administration of the study solutions (fluconazole or placebo) and the obtaining of surveillance cultures were discontinued before the determined four-week treatment period if systemic fungal infection documented, if the infant was discharged, died or transferred to another facility, or if significant hepatotoxicity was diagnosed based on biochemical monitoring. Decision on exclusion of any patient from the study and review of fungal culture pattern was done weekly. If a baby developed invasive fungal infection as determined by fungal growth in blood, solution A / B was stopped and fungal sepsis was treated with intravenous Amphotericin B. Fungal cultures were incubated aerobically at 37°C with examination for growth at 2, 5, and 7 days after plating. Those cultures with growth were further analyzed using standard micro- biologic techniques for identification of Candida species. Estimation of sample size was based on the assumption that the study would have a two-sided type 1 error rate of 0.05 or less and 84% power to detect an absolute difference of 80% in the cumulative incidence of invasive fungal infection between the placebo group and the Fluconazole group after four weeks of treatment, given a pretrial incidence of invasive fungal infection of 22%. Sixty babies were enrolled in each group. Chi square test and unpaired ‘t’ test were used to compare categorical and quantitative variables respectively. P <0.05 was considered significant. Results were analyzed using SPSS software version 11. Institutional ethics committee approved the study. An informed consent was obtained from the mother (or father) prior to enrolment. Results One hundred twenty one babies were randomized, to receive either Fluconazole or placebo, 1 baby was excluded after initial randomization (Fig.1). Demographic characteristics and baseline risk for acquisition of fungal infection in the treatment group and placebo group was similar at the time of randomization (Table I).
Table I Demographic and Clinical Characteristics of the Study Group.
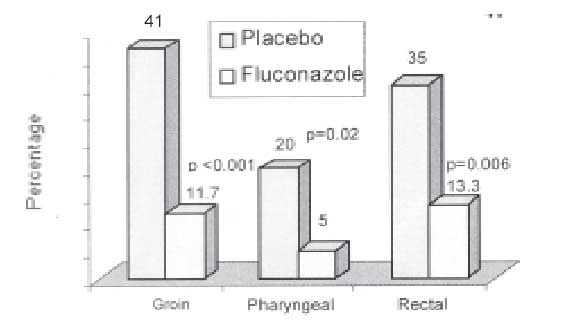
Fresh fungal colonization occurred significantly more commonly in the placebo group as compared to the Fluconazole treated group (30% vs 8.3%, P = 0.003) (Table II). Fungal species–Candida albicans, Candida parapsilosis and Candida tropicalis colonized significantly less numbers of study subjects in Fluconazole treated group (Table III). Colonization at groin, rectum and pharynx was significantly less over a period of 4 weeks in Fluconazole treated group (Fig. 2)
TABLE II Fungal Colonization in Study Subjects over 4 weeks Duration
colonization after enrolment (day 3 onwards) TABLE III Effect of Fluconazole on Colonizing Fungal Species
Invasive fungal infection was seen in 15 (25%) babies in placebo group and 16 (26.7%) babies in Fluconazole group (P = 0.835). Out of 31 patients with invasive fungal infection only 12 babies (38.7%) showed one or more clinical signs consistent with fungal infection in the preceding week (7 in Fluconazole treated and 5 in placebo treated). Out of total 31 invasive infections, Candida glabrata was the predominant species infecting 22 babies (11 babies in each of placebo and Fluconazole groups). There was no difference in the pattern of fungal isolates between the placebo and Fluconazole group (Table IV). TABLE IV Fungal Isolates in Invasive Fungal Infection
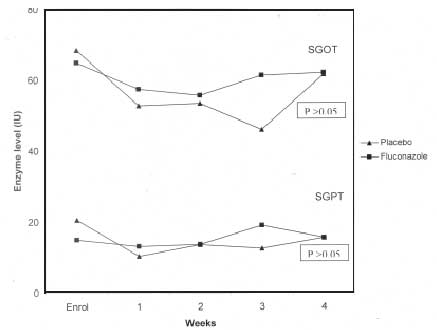
Mean age at detection of fungal invasive infection was 11.2 days (SD 5.1 ) in placebo group and 10.9 days (SD 5.7) in Fluconazole group. (P = 0.89). Preceding fungal colonization before invasive infection was seen in 7 babies (46.7%) in placebo group and 4 babies (24.6%) in Fluconazole group (P = 0.38). There was no difference in time taken to reach full feeds (12 days vs 12.8 days), days to regain birth weight (10.6 days vs 10.8 days) and total duration of hospital stay (15.7 days vs 18.0 days) in the placebo and Fluconazole treated group. Most patients developed invasive fungal infection during 2nd and 3rd week postnatally and clinical signs of fungal infection were identified only in 38.7% fungemic infants. Seventeen babies died in each of Fluconazole and placebo treated groups (P = 1). Out of 34 babies who died, 7 babies had developed invasive fungal infection prior to death (3 in fluconazole treated and 4 in placebo treated). Fungal infection was attributed as a cause of death in 4 patients (1 in Fluconazole treated and 3 in placebo treated), however, autopsy was not performed in those patients. None of the fungemic patients developed Meningitis, Endocarditis, Osteomyelitis/arthritis or Endopthalmitis. All fungemic patients started on Amphotericin B, responded well to the treatment. Fluconazole was not found to be hepatotoxic with dosage and duration used (Fig. 3).
Discussion Our study showed significantly less number of fungal colonizations in Fluconazole treated group during the 28 days surveillance period depicting protective effect on the fungal colonization by prophylactic fluconazole. In a similar study by Kicklighter, et al.(9), Candida colonization reduced from 46% to 15.1% (P <0.001) after Fluconazole therapy. In the study by Kaufman, et al.(11), Fluconazole treatment decreased incidence of fungal colonization in extremely low birth weight babies from 23% to 4.9% over 6 weeks treatment period. Fluconazole decreased fungal colonization at rectal, groin and oropharyngeal sites, that is Fluconazole was effective even at sites other than gastrointestinal tract, an advantage over use of oral local antifungals like Nystatin. Similar results were observed by Kaufman, et al., where Fluconazole decreased fungal colonization at skin, stool and nasopharynx(11). In the present study various "non-albicans Candida’ species were predominant species causing colonization (56% cases). In the study by Baley et al. and Kicklighter, et al., colonizations by "non albicans Candida" was 39% and 47% respectively(8,9). Thus when compared with previous studies, there is higher rate of colonization with non-albicans Candida in the present study. Our study demonstrated high incidence of invasive fungal infection of 25.8% in VLBW babies(1-4) with predominant fungal pathogens being non albicans Candida responsible for 96.8% cases. Study by Narang, et al. in the year 1999, from North India showed 22.8% incidence of invasive fungal infection in preterm neonates(5). Another study from the same institution showed that 56.5% fungal isolates from neonatal fungal sepsis were non-albicans candida (C. tropicalis in 21.7%, C. guillermondii in 13%, C. parapsillosis in 13% and C. krusei in 8.7%(14). In a previous study from our institution out of total 30 neonatal invasive fungal infections 46.7% were caused by non-albicans candida. (C. tropicalis (23.3%) and C. krusei (23.3%)(15). In the study by Kaufman, et al.(11) the incidence of invasive fungal infection was 20% in the placebo group and out of 10 fungal isolates 50% were non albicans candida (Candida parapsilosis 3, Candida glabrata 1 and Candida dubliniensis 1). C. krusei and C. glabrata are species with intrinsic resistance to Fluconazole(16) C.tropicalis and C. parapsilosis tend to be less susceptible to azoles, particularly Fluconazole than C. albicans(12). Clearly, present study highlights the fact that more and more cases of non-albicans candida, which are resistant to fluconazole are being isolated in our NICUs. Moreover, various Candida species which are resistant to fluconazole are now being reported. In a study by Narang, et al.(17), out of total 23 cases of fungal sepsis four isolates i.e.,17.7% (C. parapsilosis = 2, C. albicans = 1 and C. guillermondii = 1) were resistant to Fluconazole. Study from our institution showed 18.7% C. albicans isolates from neonates, resistant to Fluconazole(14). Development of resistance in Candida parapsilosis associated with long term Fluconazole prophylaxis has been demonstrated in an animal model(18). In humans, development of Fluconazole resistance in C. albicans has been demonstrated in adult HIV positive women on Fluconazole prophylaxis(19,13,20). Fluconazole is used in our NICU since last six years, which could be the reason for high incidence of non-albicans Candida species, which are less susceptible to Fluconazole. Similar timing of presentation of invasive fungal infection in the Fluconazole and placebo group highlights the fact that Fluconazole was not effective in preventing invasive fungal infection in the present study. There may be other significant factors apart from superficial colonization that contribute to fungal sepsis; as in this study, a reduction of fungal colonization by prophylactic fluconazole did not bring down rate of invasive fungal infection(9). We could not screen urinary tract for fungal infection, as it necessitates suprapubic puncture. It is likely that some cases of isolated urinary tract infection or colonization were missed. We could not test for fungal resistance to Fluconazole. Despite these two limitations, we think that routine use of prophylactic Fluconazole in very low birth weight is not recommended. Periodic review of fungal isolates is mandatory to decide unit policy on antifungal treatment. Future research should be directed to identify other risk factors for invasive fungal infection and various interventions to limit those infections. Acknowledgement KEM Hospital Staff Society, Mumbai for financially supporting the project and Dr Nilima Kshirsagar, Dean, Seth G S Medical College and KEM Hospital, for permitting to publish this article. Contributors: TP supervised sample collections and drug administration, collected and analysed the data, drafted the manuscript. RN conceptualized the study, critically revised the manuscript, will act as its guarantor. All authors contributed in development of study protocol. SR participated in data collection. CP & KB carried out the fungal tests, RU & PM supervised the study. Competing interests: None. Funding: The research project was supported by a research grant from KEM Hospital Staff Society, Mumbai.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()