|
|
Research Paper Indian Pediatrics 2007; 44:823-829 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Effect of Consumption of Micronutrient Fortified Candies on the Iron and Vitamin A Status of Children Aged 3-6 years in Rural Haryana |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
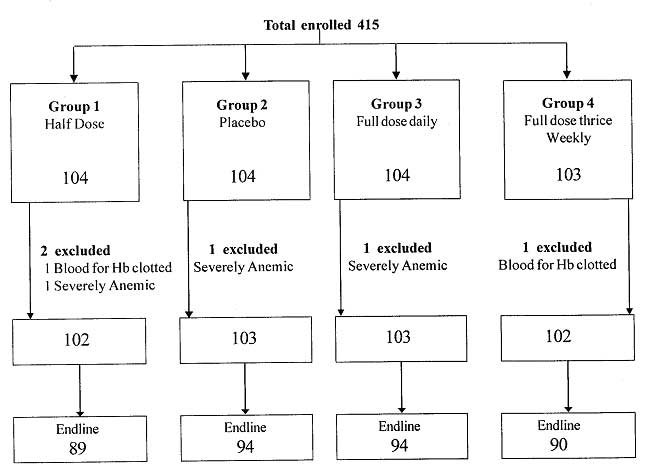
Iron and massive dose vitamin A supplementation is the most common short-term strategy currently used to control these two micronutrient deficiencies in developing countries including India. However, problems in their delivery systems and community acceptability have been documented(1,2). Food fortification is an effective and cost effective, medium-term approach to improve micronutrient status and is sustainable once established. Since the prevalence of micronutrient deficiencies are generally higher and the consequences are graver in children, the identification of a child friendly vehicle is important. Based on discussion with the Department of Women & Child Development of the Governments of India and West Bengal, the Micronutrient Initiative developed micronutrient fortified candies for use in the Integrated Child Development Services Scheme (ICDS). The primary objective of this study was to assess the efficacy of iron, folic acid and vitamin A fortified candies in improving the iron and vitamin A status after 12 weeks of intervention, in children aged 3 to 6 years. Subjects and Methods Composition of Candies The candies were center-filled with vitamin and mineral premix put in the core of the hard-boiled candy. One group received full dose (FD6) candy (vitamin A 1000 IU and 14 mg elemental iron, 50 µg folic acid and 20 mg ascorbic acid) daily, the second group received full dose candy for 3 days a week (FD3), the third group received half dose (HD6) candy (vitamin A 500 IU and 7 mg elemental iron, 50 µg folic acid and 10 mg ascorbic acid) daily and the fourth group received candies with no added vitamin and mineral (PL6). Randomization The study was carried out in 7 anganwadis and 12 preparatory schools of six villages in Ballabgarh block of district Faridabad, Haryana. A sample size of 77 children in each group was calculated to be adequate to detect an increase in hemoglobin of 0.75 g/dL among anemic children with standard deviation of 1.66(3) assuming an alpha error of 5% and beta error of 20%. Randomization was done at individual level. All children of the required age group attending the facility on that day were enrolled. The children were allocated to one of the four groups after anthropometry and blood collection based on a pre-prepared sequence in block randomization in groups of eight. Intervention The candies of different groups, undistinguishable to a naked eye, were packed in different color wrappers. The supplements were packed in pouches of six candies (for each week) and 13 pouches were prepared for each enrolled child. In the thrice-weekly group, in addition to the three fortified candies three plain candies were included to ensure blinding. This meant that the child would get three fortified candies in a week, but not necessarily on alternate days. The color codes were known to one person (SB) who was not involved in the field work and the codes were opened after the trial was over. The enrolled children had their anthropometric measurements taken by field workers using standard equipments and procedures. A record of child’s attendance and consumption of the candy was kept. Children missing a dose were tracked to their house on the same day or on a Sunday. Informed written parental consent was taken. Institutional Ethical clearance was obtained. All severely anemic children and clinical vitamin A deficient children detected during the study were given appropriate treatment and excluded from the study. All children were given hematinics and anti-helminthics at the end of study. Laboratory analysis Three mL of blood was drawn from each child. Immediately after collection, part of the sample was removed for hemoglobin estimation in an EDTA bottle and measurement of other blood morphological indicators using a blood cell counter. The remaining blood was placed on ice, protected from sunlight and centrifuged in the laboratory at Ballabgarh. The serum obtained was transferred to the laboratory at the Institute in a cold chain and used for estimation of other parameters. The biochemical parameters were measured by ELISA using kits-Hs C-Reactive protein (CRP) (Biocheck Inc. Burlingame CA BC-1119), ferritin (DiaMetra, Via Garibaldi, Italy DKO039), human retinol binding protein (RBP) (Assaypro 505135). For S. retinol measurement by HPLC, the samples were sent in a light protected environment to Molecular Diagnostic Laboratory at Lucknow. For quality control, control samples provided with the commercial kits were run with each of the batch of samples. Anemia was defined as the presence of hemoglobin levels below 11 g/dL(4,6). Low serum ferritin was defined as levels below 12 µg/L for normal children and below 30 µg/ L for children with CRP levels of more than 6 mg/mL(4). Low serum retinol was defined as below 20 µg/dL equivalent to 0.70 µmol/L(5). Data analysis The data were entered in MS Excel and analysis was done using SPSS (version 10.0). Intention to treat analysis was performed irrespective of the compliance to the intervention. The means were compared by one-way analysis of variance (ANOVA). For the variables like ferritin and retinol binding protein that were not normally distributed, logarithmic transformation was done before applying ANOVA. For comparison between two groups, Bonferoni’s post hoc test was applied. Mean change in hemoglobin and other parameters from baseline to endline were expressed as percentage of baseline values. The median value and range are presented and Kruskal Wallis rank sum test was used to estimate significance levels. Results A total of 415 children were enrolled for the study. Five of these were excluded (3 children with severe anemia and 2 due to incomplete data). At baseline, the children in the four groups were similar with respect to age, anthropometry and CRP levels but different in the sex distribution (Table I). The FD3 group had more number of girls as compared to the other groups. The prevalence of anemia was found to be 48.3% in boys and 53.9% in girls (P >0.10). TABLE I Characteristics of Study Children at Baseline
*More than 6 mg/mL A total of 42 children were lost to follow up which was higher (not significantly) for the HD6 and FB3 group (Fig. 1). The baseline characteristics of these children were not significantly different from others. The daily records showed that the intended supplementation targets were largely achieved. Minor gastric side effects were reported by 4% to 8% children including those in the placebo group. None of the children reported any major side effects.
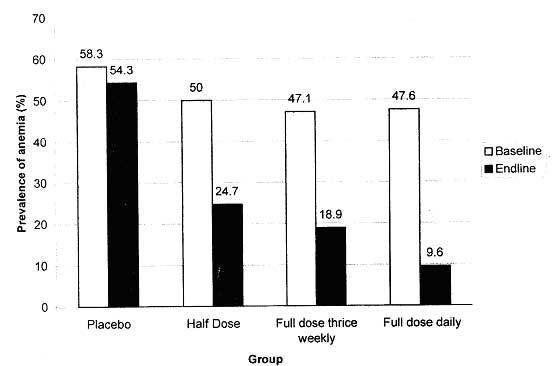
At baseline, all the parameters in the four groups were similar. At end line, mean hemoglobin levels increased significantly in all the four groups. While the increase was least in the placebo group (0.3 g/dL), it was highest in the FD3 group (Table II, Figs. 2 & 3) Correspondingly, prevalence of anemia was highest in the placebo group (54.3%) and lowest in the FD6 group (9.6%). As compared to HD6 the results for hemoglobin were better for the FD3 group even though the differences were marginal. There was no significant difference of hemoglobin levels at end line between the FD groups.
TABLE II Comparison of Baseline and Endline Values of the Biochemical Parameters in Study Children
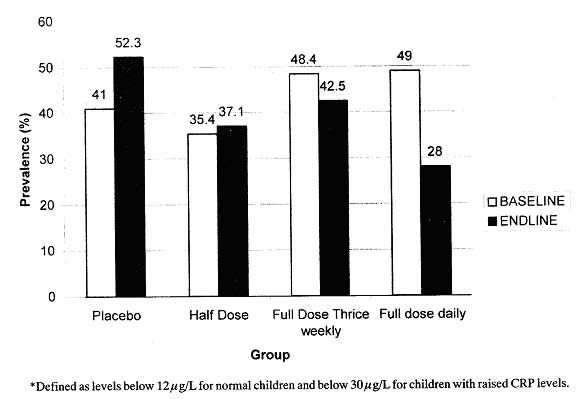
* Values expressed as Mean (SD);[n] or Median (Min, Max);[n]. # p value by Kruskal Wallis rank test. Post Hoc ANOVA a: in comparison with placebo; b: in comparison with half dose; (p<0.05) c: in comparison with full dose three times daily While baseline ferritin levels were similar, only FD6 group showed a significant rise at the end of the study indicating an improvement in the status of iron stores. S. RBP levels were similar in all the four groups at baseline as well as at endline. There was a small but insignificant increase in all the four groups at the endline. Similar to S. RBP, S. Retinol levels were also similar at baseline and end line between the four groups. The increase in S. retinol was highest for the FD6 group but was not significantly different from other groups. Sub-analysis of anemic children: The results in 208 anemic children were quite similar to the study group as a whole. At the endline, the highest mean hemoglobin levels were found in the FD6 group and the lowest in the placebo group. The mean increase in hemoglobin was about 2 g/dL in the FD group and 0.7 g/dL in the placebo group. S. ferritin levels increased at end line and were significant only in the FD6 group. The prevalence of anemia came down to 13 .3% in the children of FD6 group followed by 19% in the children of FD3 group and to one third in children of the HD6 group. Even in the placebo group it came down to 67% at endline. Sub-analysis of VA deficient children The overall prevalence of sub-clinical vitamin A deficiency was 14.2%. All the deficient children tested at end line showed an improvement of vitamin A status. However, this was not significant for the half dose group but significant in all the three other groups including placebo. Discussion This study showed that micronutrient fortified candies were successful in raising hemoglobin levels after 12 weeks of intervention in children aged 3 to 6 years. Iron stores were significantly better in the daily supplemented children. Sari, et al. conducted a trial of iron fortified candies among children aged 4-6 years in East Jakarta, Indonesia(6). This study had supplements thrice a week to ensure total of 10 candies with 30 mg of iron and 1101 IU of vitamin A per week and supplementation lasted for 12 weeks. The results were similar to this study including a significant improvement in the placebo group. In this study de-worming of all children was done before the study and could thus partly explain the increase in hemoglobin in the placebo group. In another study done in Indonesia by Schultink, et al.(7) effect of daily versus twice weekly iron supplementation (30 mg elemental iron /dose/day) on iron status was studied in pre-school children with low iron status (Hemoglobin <11g/dL). The difference in the two groups was not significant after adjustment for baseline values and daily or twice weekly iron supplementation therapy produced similar results. In our study with half that dose, it was found that daily iron therapy was much better in improving iron stores. Our intervention lasted for only 12 weeks. It is possible that a thrice weekly regimen could improve stores after a longer duration of therapy. We did not find an increase in vitamin A status of the children after 12 weeks of supplementation with a vitamin A fortified candy. As a prevalence of 15% or more of sub clinical vitamin A deficiency is required to label a community where VAD is a public health problem(5), this study area appears to be Vitamin A sufficient community. The children had not received any external vitamin A Supplementation during the study period. These candies at half doses are already being used in many states through ICDS system. Initial results from West Bengal, where effectiveness has been studied has shown positive results. This study shows that we can safely increase the dose to 14 mg of elemental iron per candy. One of the main problems facing iron supplementation program in children is that of compliance. In our study, we were able to create a "demand" for iron supplements by packing it in a candy. In West Bengal the attendance in the Anganwadi increased after the introduction of candies which also strengthened other services of ICDS as well. The candies are hard boiled candies (unlike milk based candies which stick to teeth) and the total weight of each candy is 3 grams including the premix and the wrapper. The sugar content can potentially contribute towards dental caries. So, it is important that children receive only one lozenge per day and it is followed by food supplement so that saliva can wash out the sugar. In addition, messages related to oral hygiene should be given. We had used Anganwadis and preschools for enrolling the children and these agencies also present the best way to contact these children. The actual cost of the candies at the site (including sugar, liquid glucose, primary and secondary packing, transportation, taxes and duties, etc.) comes to around twenty paise (INR 0.20) per candy. The cost of delivering the candies through the health worker is likely to be similar to that of vitamin A capsule at nine paise per beneficiary(8). Thus, the approximate cost of delivering one candy fortified with four micronutrients to a beneficiary comes to about 29 paise (INR 0.29). If about 100 candies are distributed per year to a child, this comes to about INR 29 per child per year. This appears to be a cost-effective way of addressing anemia. We, therefore, believe that micronutrient fortified candies present a potentially innovative public health tool for prevention of anemia in children. Acknowledgement We are grateful to Dr Ujjwala Godbole from Molecular Diagnostic Laboratory, Lucknow for estimation of S. retinol levels of the children. Contributors: KA designed the study, supervised the data collection, planned the analysis, drafted the manuscript and is the guarantor of the paper. RL & VNJ were responsible for the all laboratory work and reviewed the manuscript. Ritvik organized field work, data management, and performed the statistical analysis; PM & SKK supervise the field work and provided inputs on the design, conduct and drafting of the paper; RMP generated the random allocation sequence, and inputs on statistical analysis. RS & SB conceived the study, provided inputs for design and reviewed the manuscript. Competing interests: None. Funding: Micronutrient Initiative Asia.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
![]()