|
|
Lead Article Indian Pediatrics 2007; 44: 817-822 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Vitamin K1 versus Vitamin K3 for Prevention of Subclinical Vitamin Deficiency: A Randomized Controlled Trial |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
D. Chawla, A.K. Deorari, R. Saxena*, V.K. Paul, R. Agarwal, A. Biswas* and A. Meena*
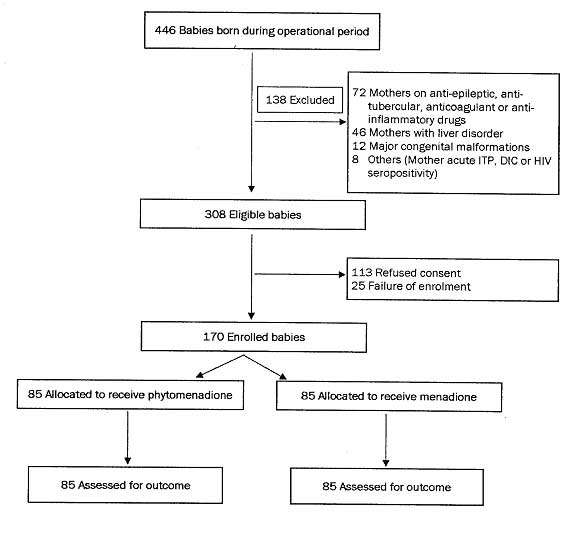
The efficacy of neonatal vitamin K prophylaxis (oral or parenteral) in the prevention of early ‘vitamin K deficiency bleeding’ (VKDB) has been firmly established by observational studies, clinical trials, and meta-analysis(1-6). Although fat soluble form of vitamin K (vitamin K1, the preparation used in most clinical trials demonstrating efficacy of neonatal vitamin K prophylaxis and is thought to cause less hemolysis than water soluble vitamin K) is the recommended preparation for neonatal prophylaxis, water soluble form (vitamin K3, less expansive and more easily available in India) is still the most widely used preparation in developing countries. No trial till date has compared relative efficacy of water soluble vitamin K (K3) and fat soluble vitamin K (K1) in prevention of vitamin K deficiency. We conducted a double-blind randomized trial to compare the efficacy of vitamin K1 and vitamin K3 in prevention of sub-clinical vitamin K deficiency. and to determine if vitamin K3 results in more hemolysis than vitamin K1. Subjects and Methods The study was carried out as a double-blind randomized controlled trial at a tertiary care center. All inborn healthy term ( ≥37 completed weeks) appropriate for gestation neonates were eligible for inclusion in the trial if parents lived within 20 km distance from the hospital and the birth occurred during operational period of the study. Operational period was defined as the period when primary investigator (DC) was posted in clinical services and birth occurred from 9 am to 9 pm on working days. Exclusion criteria were unwillingness of family to participate in the study; mothers on anti-epileptic, anti-tubercular, anticoagulant or anti-inflammatory therapy or mother had received vitamin K within 7 days of delivery; mothers with liver disorder; any prenatally diagnosed bleeding disorder; major congenital malformation or requirement of intensive care for more than 48 hours.The subjects were randomized using a computer-generated list in fixed blocks of four each. Random treatment assignment was placed in serially numbered, opaque and sealed envelopes to conceal the treatment group allocation. Investigators providing clinical care, laboratory personnel and investigator performing statistical analysis were blinded to treatment group allocation. Enrolled subjects were randomized to receive 1 mg of either phytomenadione (vitamin K1, Inj. Kenadion, Samarth Pharma India, Group I) or menadione (vitamin K3, Inj. Kapilin, GlaxoSmithKline Pharmaceutical Limited, Group II) intramuscularly on antero-lateral aspect of thigh. Ampoules of these injections were wrapped in a paper and then placed singly in serially numbered opaque envelopes. After obtaining consent from parent(s) of an eligible baby, the sealed envelop was handed over to on-duty nurse and she was instructed to open the envelope and give the injection on antero-lateral aspect of thigh. Exclusive breast feeding was advocated for all the babies in the study. Non-carboxylated form of coagulation factors II is commonly used as a marker of vitamin K deficiency and is referred to as ‘protein induced in vitamin K absence’ (PIVKA-II). Primary outcome of the study was ‘detectable PIVKA-II’ at 72 ± 12 h of life. PIVKA-II level of >2 ng/mL was considered as ‘detectable’. A blood sample was drawn by venepuncture from all study subjects at 72 ± 12 hours of age and used for estimation of PIVKA II, total serum bilirubin (TSB) and packed cell volume (PCV). PIVKA II was estimated by ELISA using Asserachom PIVKA II (DeCarboxy Prothrombin) kit (Diagnositca Stago, France). The PIVKA II assay was performed on plasma using a murine monoclonal antibody available in an enzyme immunoassay kit (Asserachrom PIVKA-II; Diagnostica-Stago, Asnieres Sur Seine, France) (7). Secondary outcome variables were TSB level at 72 ± 12 of age, PCV at 72 ± 12 of age and any clinical bleeding within 72 h of age. PCV was measured by rotating blood-filled capillaries. TSB was estimated using twin-beam microbilimeter (Ginevri, Rome, Italy) which works on the principle of spectrophotometry. Prevalence of PIVKA-II presence in neonates given intramuscular vitamin K3 has been reported to be around 30%(8,9). A sample size of 90 each group was required to detect a difference of 20% with confidence of 95% and power of 90%. Data entry and analysis was done using Epi-info 2004 software. Continuous data with normal distribution was analyzed by Student t-test and non-normally distributed data by Wilkoxson’s Rank Sum test. Categorical data was analyzed by chi-square test. P value of <0.05 was taken as significant. The study was approved by the Ethics Committee of the hospital, and an informed written consent was taken from parents of all included subjects. Results Figure 1 details the inclusion and randomization of the study subjects. Enrolled subjects (n = 170), and those excluded due to refusal to participate (n = 113) had similar gestation (38.4 ± 1.0 wk vs 38.6 ± 1.0 wk; P = 0.54) and birth weight (2936 ± 315 g vs 2954 ± 410 g; P = 0.35). Table I compares the baseline variables between Group I and Group II. PIVKA-II levels were >2 ng/mL in 48.2% (41/85) babies in Group I (phytomenadione) and 44.7% (38/85) babies in Group II (menadione) (relative risk 1.1; 95% confidence interval 0.8 to 1.5, P = 0.76). In Group I, 84.6% (72/85) neonates, and in Group II, 94.1% (80/85) babies had PIVKA-II levels <3 ng/mL. Five neonates (5.9%) in Group I had PIVKA-II levels >10 ng/mL of which, 3 (3.5%) had PIVKA-II >100 ng/mL. No baby in Group II had PIVKA-II more than 10 ng/mL. Other outcome variables between the groups are compared in Table II. Four (4.7%) neonates in Group I and seven (8.2%) neonates in Group II had TSB ≥12 mg/dL (P = 0.53). No subject in either group had clinical bleeding up to 72 hours of age.
TABLE I Baseline Variables of Enrolled Subjects
Values are expressed as mean (SD); *median (range); †number (percentage). TABLE II Main Outcome Variables
PIVKA: Protein Induced in vitamin K absence–II; *mean (SD); †median (IQR).
Discussion We have compared efficacy of vitamin K1 and vitamin K3 in preventing sub-clinical vitamin K deficiency in a double-blind randomized controlled trial, and have shown that at 72 ± 12 hr of age, PIVKA-II values did not differ significantly between the two groups. Presence of PIVKA-II in blood is a highly specific and sensitive marker of vitamin K deficiency compared to prothrombin time (PT). Babies who do not receive prophylactic vitamin K at birth have high detection rate of PIVKA-II at 72 hr of age(8,10). Considering PIVKA-II level more than 2 ng/mL as abnormal (as advised by manufacturer of the PIVKA-II estimation kit used in the study), almost half of the subjects in both the groups had sub-clinical vitamin K deficiency despite receiving adequate prophylaxis. Such a high rate of PIVKA-II detection in babies receiving vitamin K prophylaxis has not been reported in published literature. Motohara, et al. (11) used a cutoff value of abnormally elevated PIVKA-II as a level more than 0.1 AU (Arbitrary Unit)/mL. They detected PIVKA-II in 21.5% of cord blood samples. At 3 to 5 days of age 50-60% of infants were PIVKA-II positive if they were breastfed and had not received vitamin K prophylaxis at birth. von Kries, et al.(10) also defined PIVKA-II more than >0.1 AU/mL as abnormal and reported 48% detection rate in control and none in supplemented group. Sharma, et al.(8) in their prospective study on 51 term, healthy breastfed newborns measured PIVKA-II levels in cord blood and at 72-78 hours of age. Comparison of PIVKA-II results in current study with those of previous studies is hampered by the fact that our method of PIVKA-II estimation was more sensitive. Their detection limit amounted to 0.10 to 0.13 Arbitrary Unit per mL (1 AU = 1 µg purified prothrombin = 1000 ng/mL) compared to up to 1 ng/mL in our study. Secondly, some of the PIVKA-II activity at 72 hr of age might arise from intrauterine vitamin K deficiency. Greer, et al.(12) in a study found PIVKA-II level equal to or more than 0.1 AU/mL in 48% of cord blood samples. By sequential measurements of PIVKA-II activity half life of PIVKA-II was calculated to be 45-50.8 hr. Thus, using a highly sensitive test may detect the PIVKA-II of fetal origin and decrease its specificity for detection of subclinical vitamin K deficiency. We did not measure PT in this study. PT is abnormal only in severe vitamin K deficiency state (less sensitive than PIVKA-II) and can be prolonged even in deficiency of non-vitamin K dependent coagulation factors (less specific). Furthermore, assessment of coagulation factors in the newborn infant is complicated by the fact that ‘normal’ plasma concentrations of these factors are 30-60% of adult concentration. High PIVKA-II detection rate in both groups raises questions about adequacy of recommended dose of 1 mg in preventing subclinical vitamin K deficiency. Presently, recommended dose of 1 mg has been arrived at based on observational data and may require finer refinement. Such an adjustment in dosage should be carried out only on the basis of a large randomized controlled trial. Pharmacogenetics variation or polymorphism of genes encoding the enzymes involved in synthesis of vitamin K-dependent coagulation factors (e.g., vitamin K epoxide reductase complex 1) can be another factor responsible for Indian neonates requiring a different dose of vitamin K than their Western counterparts(13). Although, investigating the same was outside the scope of the present study, a further investigation into the phenomenon is needed. Although five (5.9%) babies in Group I (vitamin K1) had PIVKA-II more than 10 ng/mL compared to none in Group II, this difference was not statistically significant (P = 0.07). Three babies in Group I had PIVKA-II levels more than 100 ng/mL. Although such a high level of PIVKA-II may indicate more severe vitamin K deficiency in vitamin K1 group, our study was not powered enough to detect such a small difference between the two groups. Absence of any episode of clinical bleeding in our study is not unexpected as clinical vitamin K deficiency is a rare event and sample size required to detect any difference in clinical bleeding is much larger. Vitamin K3 has gone out of favor in most parts of the world because of fear of hemolysis. However, it continues to be in use in view of easy availability and low cost in developing countries. In present study we did not find any difference in mean TSB (7.3 vs 7.6 mg/dL) or PCV (53.1% vs 54.2%) at 72 ± 12 hours of age. Four (4.7%) babies in Group I and 7 (8.2%) babies in Group II had TSB ≥12 mg/dL and this difference was not significant (P = 0.53). In an earlier study at our institute(9), we used vitamin K3 to compare its efficacy through oral and intramuscular routes and did not find any pathological hyperbilirubinemia attributable to use of vitamin K3. It appears that routine dose of vitamin K does not result in significant hemolysis. Vitamin K-induced hemolysis is mediated through oxidant injury and one contributing factor can be coexisting glucose-6-phosphate dehydrogenase (G6PD) deficiency. We did not screen our babies for G6PD deficiency. One shortcoming of the study was exclusion of large number of babies due to refusal to participate in the trial. But excluded group was not different from enrolled group of babies as per birthweight and gestation age. Comparable PIVKA-II detection rate and PIVKA-II levels in neonates receiving phyto-menadione or menadione indicate similar efficacy of two preparations of vitamin K. High PIVKA-II detection rate observed with both preparations indicates recent vitamin K deficiency and may be due to either inadequate dose of vitamin K or persistence of PIVKA-II of fetal origin. Current recommendation of using a dose of one mg may not lead to significant hemolysis with either of the preparations. Contributors: DC had primary responsibility for protocol development, patient screening, enrolment, outcome assessment, preliminary data analysis and writing the manuscript. AKD, RS, VKP and RA participated in the development of the protocol, in supervising enrolment and writing of the manuscript. AB & AM participated in outcome assessment. Funding: Purchase of PIVKA kit was funded by Institute Research Grant, All India Institute of Medical Sciences. Vitamin K injections were provided by Samarth Pharma Pvt. Ltd, India. Manufactures of vitamin K1 or K3 were not involved in design, conduct, analysis, interpretation or decision of publication of the study. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()