|
|
Case Reports Indian Pediatrics 2006;43:994-997 |
||||
|
Ischemic Stroke Following Mild Head Injury: Is it the Cause? |
||||
|
K.S. Rana From the Department of Pediatrics, Armed Forces Medical College, Pune, Maharashtra, India. Correspondence to: Lt. Col. K.S. Rana, Associate Professor of Pediatrics and Pediatric Neurology, Armed Forces Medical College, Pune, India. E mail: kamersinghrana@yahoo.co.in Manuscript received: October 18, 2005; Initial review
completed: November 5, 2005;
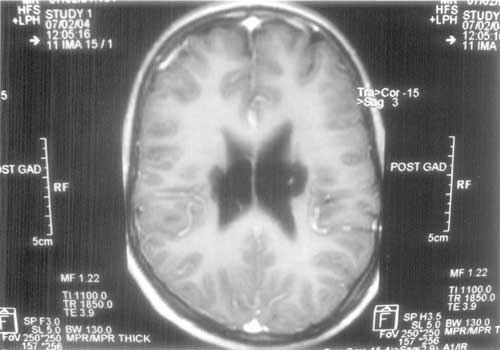
Recognition of childhood stroke is difficult and challenging. Annual average reported incidence in India is 13-33/100,000 per year(1). Head trauma usually causes hemorrhagic stroke. Spontaneous intra-cerebral bleed or bleed following mild head injury usually occurs in association with vascular abnormalities or coagulopathies and there is high risk of recurrence(2). We are presenting seven cases of ischemic stroke following mild head injury. Case Reports Case 1 An 11-month-old male infant had a fall from his mother’s lap while feeding. Next day he was not moving his left half of the body. There was no history of altered sensorium, vomiting, altered sleep, seizure, fever, drug intake or bleeding from anywhere. Examination suggested left upper motor neuron 7th nerve palsy and left hemiparesis. CT scan done on 3rd day suggested ischemic infarct involving right internal capsule and basal ganglia. He completely improved with physiotherapy. On day 9th again he had a fall from a small chair in the hospital and this time developed hemiparesis on right side after 2 hr. He was extensively investigated for the cause of recurrent stroke. Investigations included routine blood, bleeding and coagulation profile, peripheral smear, test for sickle cell disease, arterial blood gases, serum lactate, urine for amino acids, lipid profile, CSF studies including PCR for tuberculosis, X-ray chest, echocardiography, electrocardio graphy, electroencephalography, antinuclear antibodies, antiphospholipid antibodies, blood homocystiene and mountex test. All investigations were normal. MRI brain suggested infarct involving bilateral basal ganglia, internal capsule and periventricular white matter (Figs. 1a & 1b). MRA was normal. This time also he improved completely. Subsequent follow up after one year revealed mild dysarthria and bilateral extensor plantar. Patient could not afford estimation of protein C and S , Factor 5 Lyden and anti thrombin III.
Case 2 A 12-year-female child developed left hemiplegia at the age of 10 mo, following a fall. At one year of age again after a fall while walking on the floor, she developed right hemiplegia. Examination revealed dysarthria and bilateral upper motor neuron signs. MRI, done after 3 days of the fall, suggested ischemic infarct involving bilateral basal ganglia and internal capsule. MRA was normal. Case 3 An 1-month-male child developed right hemiparesis after a fall from the bed. CT brain done after three days showed ischemic infarct in left basal ganglia and internal capsule. Investigations were normal. After three months child was able to walk but while running he was having frequent falls. Examination at that time suggested brisk DTRs and extensor plantar on right. Case 4 An 18-month-male child was born out of 2nd degree consanguinity. He developed right hemiparesis after a fall from bed. CT brain done after five days, suggested ischemic infarct involving left basal ganglia and internal capsule. Investigations were normal. After 5 mo he was having no symptoms, tone was normal but DTRs on right side were brisk. Case 5 A 4-year-male child developed right hemiparesis after a fall while playing. MRI suggested subacute ischemic infarct left basal ganglia and corona radiata. MRA was normal. After six months, he was asymptomatic but upper motor neuron signs persisted on the right side. Case 6 A 6-year-male child had a fall from bed at six months of age. He developed right hemiparesis after one month and partial motor seizures after six months. He is still on sodium valproate and is seizure free. Examination revealed microcephaly. CT brain done after a month, showed ischemic infarct involving left internal capsule and parietal lobe. Case 7 4-year-male child developed right hemiparesis and right focal motor seizures after a trivial fall at eight months of age. CT brain done seven days after the fall showed old infarct involving left parietal lobe, internal capsule and basal ganglia. The child had microcephaly (head circumference 44 cm). Discussion Cranial trauma in young children can cause ischemic infarct(3-6). This is an unusual mechanism of childhood stroke and should be considered after systematic exclusion of other causes. All our children were less than five years of age at the time of presentation; and all had trivial fall. In all except one, the deficit was observed after a gap of 12 hrs. Other adverse neurological consequences following mild head injury in children can be migraine, encephalopathy, seizures and focal neurological deficit(7). Rarely a malignant syndrome, characterized by delayed cerebral edema and coma is also seen. Children with this dangerous entity have mutation in the CANAIA calcium channel subunits gene(8). This association also suggests the possible role of genetic susceptibility in young children presenting as stroke after mild head bang. The pathophysiology of stroke after mild head injury in young children is either thrombus or spasm of lenticulostriate branches of middle cerebral artery. These vessels are end arteries and after originating from the main trunk at an acute angle (more acute in young), follow a recurrent course before penetrating the anterior perforated substance. There is, therefore a redundant extra cerebral segment. Any motion of the brain may lead to disruption of the arteries between the mobile extra cerebral segment and the fixed intra cerebral portion. This may lead to mechanical disruption of distal blood supply or intimal trauma and subsequent thrombosis or spasm(2,9). Relative delay of symptoms in most of cases can be explained on the basis of thrombus generation and immediate onset in two probably because of mechanical disruption of blood or spasm. Viral infection particularly varicella causes vasculopathy and susceptibility to develop arterial thrombosis or spasm following mild head injury(10). Such history was not there in our cases. Four children developed their symptoms during the months of April and May suggesting some common environmental factor, may be sub clinical viral infection predisposing them for ischemic stroke following mild head injury. The temporal relationship of stroke with mild head injury, clustering of cases during pre monsoon period and exclusion of other common causes of stroke may suggest that mild head injury leading to ischemic stroke in association with common environmental factor like viral fever is not merely coincidental. Detailed history of the days before the stroke may identify more traumatic events in young children especially in the group of so called idiopathic strokes. However more studies are required to understand the susceptibility, environmental and genetic factors and pathophysiology of this entity. Contributors: All authors were involved in managing the patients and preparing the manuscript. Funding: None. Competing interests: None stated.
| ||||
|
References | ||||
|
|
![]()