|
|
Personal Article Indian Pediatrics 2006; 43:953-964 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Total Parenteral Nutrition in Neonates |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
From the Department of Pediatrics, KEM Hospital, Pune 411 011, Maharashtra, India Correspondence to: Dr. Sudha Chaudhari, Consultant, Division of Neonatology, Department of Pediatrics, KEM Hospital, Pune 411 011, Maharashtra, India. E-mail: kemhrc@vsnl.com
Total Parenteral Nutrition (TPN) may be defined as provision of nutrition for metabolic requirements and growth through the parenteral route. The concept of parenteral nutrition existed way back in 1660 when oils and wines were given intravenously(1). The importance of protein administration for nitrogen balance, weight gain and general well being was demonstrated as early as 1852 by Bidder and Schimdt(2). In 1966, Dudrick made a major discovery by implanting a catheter in the superior vena cava of beagle puppies(3) and subsequently in an infant with short bowel syndrome and gave parenteral nutrition(4). He summed up the indications for TPN very simply, by saying that it should be given in babies "who cannot eat, should not eat and cannot eat enough." Parenteral nutrition has become increasingly complex. Careless use due to inadequate understanding or poor supervision, can result in devastating complications like septicemia and metabolic imbalances. To maximize benefits and minimize complica-tions, many medical centers have developed a team approach to parenteral nutrition. However, in the Indian situation, the physician has to take over all the roles of the entire team. Total Parenteral Nutrition is technically demanding, expensive and has several side effects. Hence, its use is only justified when enteral feeding is impossible. Its duration should be as short as possible and at least partial enteral feeding should be started as early as possible. TPN should only be used in units where (i) there is full time medical coverage, (ii) trained nursing staff who can be relied upon for proper care of IV lines, (iii) facilities to prepare solutions correctly under laminar flow hood (iv) appropriate laboratory backup and (v) appropriate equipment including infusion pumps. In 1986, we investigated the feasibility of using TPN in neonates and children in a developing country like ours, the cost involved, the problems encountered and the means to circumvent these problems(5). Use of TPN in neonates The nutritional requirements of extremely low birth weight infants (ELBW) are rarely met with and they lose a lot of weight in the first two weeks of postnatal life. Early use of parenteral nutrition may minimize these losses and improve growth outcomes. Parenteral nutrition solutions have improved markedly from the early days of use in the 1980’s and complications are now less common. In general, five or more days without adequate nutrition in full term neonates or three or more days without nutrition in VLBW infants places them at nutritional risks and would be an indication for prophylactic TPN. TPN is indicated when neonates cannot tolerate enteral feedings or when there is a need to supplement enteral intake. The indications for TPN are given in Table I. Components of TPN solutions The infusate should contain the following:- TABLE I Indications for TPN
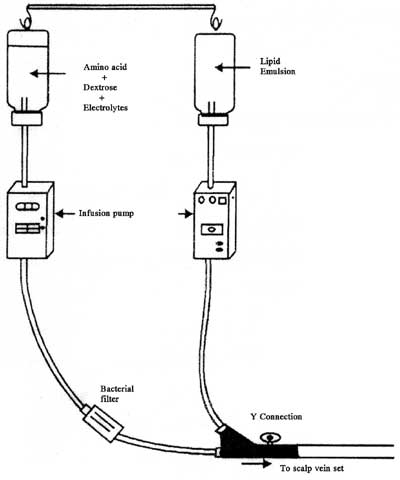
(1) Protein as crystalline aminoacids. (2) Fats as lipids. (3) Carbohydrate as glucose. (4) Electrolytes–Sodium, potassium, chloride, calcium and magnesium. (5) Metals/Trace elements–Zinc, copper, manganese, chromium, selenium. (6) Vitamins A, C, D, E, K, thiamine, riboflavin, niacin, pantothenic acid, pyridoxine, biotin, choline and folic acid. Fluids Fluids are a very essential part of parenteral nutrition. Volumes should be increased over the first 7 days depending on electrolytes, hydration and clinical status with the aim of delivering 150 mL/kg/day by the end of a week. Energy requirements The most important goal of parenteral nutrition is to provide sufficient energy and nitrogen to prevent catabolism and to achieve a positive nitrogen balance. Preterm infants have very low energy reserves due to low amounts of fat as well as low glycogen reserves in the liver. The ideal distribution of calories should be 60% carbohydrate, 10-15% proteins and 30% fats(1). A 10% dextrose solution provides 0.34 kcal/mL. A 10% lipid solution provides 0.9 kcal/mL. Although protein is a potential energy substrate, it should be utilized only for tissue growth. Glucose and lipids should provide sufficient calories to avoid protein catabolism. A preterm neonate needs 100-150 kcal/kg/day, whereas a term neonate needs 100-120 kcal/kg/day. Carbohydrate requirements Glucose is the most widely used intravenous carbohydrate for neonates because it is readily available to the brain. A preterm infant, who may have hypothermia and respiratory distress, has a higher glucose demand and hence early administration of glucose is vital(6,7). It is important to balance non-protein calories between carbohydrates and fats. Excess use of glucose would result in lipogenesis, excess production of CO2 and hyperglycemia, which may produce osmotic diuresis. Protein requirements The goal in giving proteins is to limit catabolism and maintain endogenous protein stores, and to provide sufficient energy and protein intake to support growth. In an article entitled "Aggressive nutrition of the VLBW infant," Ziegler, et al.(8) state that early administration of PN today is safe and efficacious and no longer fraught with metabolic derangements that had at earlier times made PN a dangerous proposition in VLBW infants. The concept put forth by American Academy of Pediatrics(9) that "nutrition should support postnatal growth that approximates the in utero growth of a normal fetus" should be accepted. Protein is delivered as a synthetic amino acid solution, which gives 4 kcal/g. These solutions contain 9 essential amino acids and cysteine, tyrosine, taurine and arginine as the semi-essential amino acids. In the absence of an exogenous protein source, a preterm infant will catabolise 1 g/kg/day of their own body protein to meet its metabolic needs. Excess protein administration will cause a rise in blood urea, ammonia and high levels of potentially toxic amino acids such as phenyl-alanine. Paisley and Thureen(10) started amino acids in a dose of 3 g/kg/day within 24 hours in ELBW infants. They showed that higher amino acid doses led to significantly higher protein balance. The experience with this high dose of amino acids is limited and some caution is warranted. In our unit, we start amino acids on the second day of life for ELBW infants with 1 g/kg/day and go upto 3 g/kg/day with daily increments of 1 g/kg/day. Some units start smaller doses of amino acids in septic or hemo-dynamically unstable babies. A maximum of 15% calories should be given as proteins. Lipids Lipids are a major source of non-protein energy and have a nitrogen sparing effect. It serves as a source of essential fatty acids as well as long chain polyunsaturated fatty acids (LC-PUFA). The importance of LC-PUFA for the development of the brain and retina is well known. The commercial IV lipid emulsions are aqueous suspensions containing neutral triglycerides derived from soybean, safflower oil, egg yolk to emulsify and glycerine to adjust tonicity. Hydrolysis of triglycerides by hepatic and lipoprotein lipase results in formation of free fatty acids. The free fatty acids circulate and can be used as an energy source or they can enter adipose tissue, where they are re-esterified to form triglycerides(11). Early use and rapid advancement of lipid emulsions in premature infants should be done cautiously because of a variety of potential complications and toxicities. These are lipid intolerance, increased free bilirubin concentrations, impaired pulmonary function, increased risk for developing chronic lung disease and interference with immune and platelet function. If free fatty acids accumulate, they can displace bilirubin from albumin(12). There has been concern that intravenous lipids induce thrombocytopenia. However, present data does not support this notion(13). Early investigators suggested that intravenous lipid emulsion impaired neutrophil function, but more recent studies have demonstrated normal immune function(14). There is a theoretical risk involved in giving lipids in a neonate with severe respiratory distress due to fear of pulmonary embolism and PGI2 formation, which may cause ventilation/perfusion mismatch(15). However, lipids when given as a slow infusion over 24 hours are not associated with worsening of respiratory distress. Both 10% and 20% formulations are available. When lipids are exposed to light, they form potentially toxic lipid hydro-peroxides. Hence lipid syringes and tubing should be covered by wrapping it in foil or carbon paper if foil is not available(16). It should be given by a separate line (Fig.1). Due to their isotonicity, they can be given through the peripheral line. The tolerance for lipids in extremely premature infants is often poor and hence triglyceride levels should be monitored closely. The dose of lipids may be reduced following acute episodes of sepsis, respiratory distress, thrombocytopenia and severe hyper-bilirubinemia.
In our unit, we usually start lipids on the third day of life in ELBW infants when the most acute phase of respiratory distress or other life threatening events is controlled. We start with 1 g/kg/day and go upto 3 g/kg/ day with increments of 1 g/kg/day. At present 20% lipid emulsion is preferred over 10%, because the higher phospholipid content of the 10% solution impedes plasma triglyceride clearance, resulting in higher triglyceride and plasma cholesterol concentration. Advantages of lipid emulsions over concentrated glucose solutions include their isotonicity and greater energy density, the latter meaning that less volume is required per calorie. This is particularly true for 20% lipid, because it leads to a more normal pattern of plasma lipids in ELBW infants. We use 10% lipid solutions because 20% lipid solutions are available only in 250 mL bottles and not in 100mL bottles. Not only is the cost more, but there is a lot of wastage of the lipid solution since ELBW babies need such a small quantity. There is really no credible evidence of adverse effects when IV lipids emulsions are used properly. Proper use includes slow infusion rates (<150 mg/kg/hr) and avoidance of unduly high doses i.e., >3g/kg/day. Minerals Sodium, potassium, chloride, calcium, magnesium and phosphorus levels need to be closely monitored and the infusate needs to be prescribed accordingly. Trace elements Trace elements like zinc, copper, manganese, selenium, fluorine and iodine are provided in some of the TPN solutions available abroad. However, the Indian TPN solutions do not contain these trace elements. Neonates on long term TPN may develop trace element deficiencies and it is recommended that their levels should be checked(17). In general we use only short term TPN and hence do not add trace elements. Vitamins The daily requirements for both water and fat-soluble vitamins can be provided in TPN. The dose of Pediatric Multi vitamin Infusion is 1 mL/kg/day, with an absolute maximum of 5 mL/day. This should be added to the dextrose-electrolyte solution. Other additions Heparin may be added to the TPN solutions in 0.5-1 unit per ml to decrease the risk of thrombosis. Use of heparin is recommended in neonates where small lumen central lines are used. Its use is contraindicated in neonates with evidence of coagulopathy. Table II shows the calculation of TPN step by step. TABLE II Step for Calculation of TPN
Illustrative case (For TPN calculation) A 5-day-old neonate, with gestational age of 28 weeks and birth weight of 900 g with respiratory distress on a ventilator, on TPN since day one. Step I: Total fluids 150 mL/kg = 135 mL Step II: Aminoacid (10%) 3 g/kg/day = 27 mL Step III: Lipids (10%) 3 g/kg/day = 27 mL Step IV: Supplementation (1) Sodium 3 meq/kg/day = 2.7 meq Conc. Ringer lactate = 0.9 mL (2) Potassium 2 meq/kg/day = 1.8 meq Potassium chloride = 0.9 mL (3) Calcium 2 meq/kg/day = 1.8 meq Calcium gluconate 10% = 4 mL (4) Magnesium 0.3 meq/kg/d = 0.27 meq 50% Magnesium sulphate = 0.07 mL (5) MVI 1 mL/kg/day MVI solution = 0.9 mL Step V: Dextrose Infusion: 6 mg/kg/min = 7.8 g/24hours Total fluids – Total additives (Step II, III, IV) 135 – 60.77 = 74.23 mL This can be given as 10% dextrose 70 mL = 7000 mg 50% dextrose = 1.6 mL = 800mg Distilled water = 2.63mL = 0 mg Step VI: Calculation of Caloric Nitrogen Ratio Total carbohydrate calories + Total fat calories × 6.25 ¸ Amino acid (g) (7.8 × 3.4) + (2.7 × 9) × 6.25 CNR = 117.63 cal/g Step VII: Add heparin 1 unit/mL = 135 units Note: If the baby is unstable, calculations may have to be done every 12 hours instead of every 24 hours. TPN preparation All the TPN bottles are kept in laminar flow hood and ultraviolet rays are switched on. Two hours later, the ultraviolet rays are switched off. The doctor or nurse scrubs and puts on a gown, cap and mask and gloves and mixes the solutions as per calculation inside the laminar flow hood. If ultraviolet rays are not switched off during mixing, the personnel may get conjunctival irritation. They then connect the bottles to the IV set under strict aseptic precautions. The TPN assembly is shown in Fig.1. The bottles along with the tubing are changed every 24 hours. Peripheral versus central venous access PN is delivered by peripheral or central vein access, depending on the concentration of dextrose and consequent osmolarity of the solution. The maximum concentration of dextrose for peripheral venous access is 12.5%. A dextrose concentration greater than 12.5% has an acidic pH and can be irritating to the peripheral veins. In addition to dextrose, electrolytes and minerals added to the solution increase the osmolarity of the solution. Short term TPN for less than 3 days can be given via the peripheral line. Hypertonic solutions must be administered via a central venous catheter to prevent peripheral vein inflammation and thrombosis. There are no restraints on the osmolarity of central PN because of its high flow rate, infusion into a large vessel and the type of catheter used for infusion. PN can be given through the umbilical vein. Route of administration TPN should be delivered whenever possible through central lines. Usually, a percutaneous central line is placed with the position of the tip of the catheter confirmed by X-ray. The amino acid solution is attached to a burette with a suitable bacterial filter in line with a Y connector to which the lipid infusion is attached (Fig.1). A strict aseptic technique in preparation and administration of TPN is mandatory. Breakage of the central line through which TPN is administered should be avoided. Drugs should be given through a separate IV line. Monitoring protocol for parenteral nutrition Meticulous monitoring is necessary not only to detect complications, but to document clinical benefit(18). Most septic and metabolic complications can be prevented or detected before they cause serious consequences, if the monitoring protocol is followed rigidly. Monitoring should be more frequent in the initial stages. Once a steady metabolic stage has been achieved, monitoring can be reduced to once a week. Table III gives the monitoring protocol of neonates on PN in our hospital. It is essential to develop micromethod systems for biochemical monitoring of infants. In the absence of these, blood sampling volumes should be carefully recorded and replenished. Adjustment of daily electrolytes, nutrients and fluid orders are based on biochemical monitoring. TABLE III TPN Monitoring Schedule
Source: Protocol of KEM Hospital, Pune. Complications Sepsis is the most common and serious complication of TPN in India. In 1986, we reported an incidence of 52% of sepsis in 36 patients given TPN(5). But twenty years later, our sepsis rate has gone down considerably with the use of laminar flow hood for preparation and training of nurses in strict aseptic techniques. Table IV summarizes TPN related complications. TABLE IV
Dextrose related complications Hypo and hyperglycemia are more common in neonates than older children and hence blood glucose should be monitored closely. Dextrose infusion should be cut down if hyperglycemia occurs. Treatment of hyperglycemia is initiated with insulin if blood glucose is above 200 mg/dL despite reducing the dextrose infusion below 5 mg/kg/min. Insulin can be started in a dose of 0.05-0.1U/kg/hr(19). Adjust insulin infusion rate by 0.05 U/kg/hr to keep glucose levels to 150-200 mg%. Discontinue when levels drop to <100 mg% and monitor glucose every 4 hours once target level is achieved. Before starting insulin, rule out other causes of hyperglycemia like sepsis, intraventricular hemorrhage, steroids. Protein related complications If BUN is raised twice above the normal value, fluids may have to be increased or protein may have to be cut down(6). Lipid related complications Hyperlipidemia and hyperbilirubinemia may occur in neonates. Lipids may have to be cut down or stopped completely(20). PaO2 may be lowered due to changes in pulmonary microcirculation, especially in neonates with RDS. Lipids will have to be stopped if there is severe sepsis. Severe sepsis is defined as sepsis with organ dysfunction associated with hypotension and need for inotropes. Hepatic effects Liver disease due to PN is a well-recognized iatrogenic entity, also called PN associated cholestasis. PN associated cholestasis is defined as onset of hyper-bilirubinemia within 2 weeks of starting PN(21). Thureen, et al. have stipulated that a direct bilirubin >2 mg/dL may be called cholestatic jaundice(22). There may be hepatomegaly, mild elevation of conjugated bilirubin, alkaline phosphatase and transaminases. Liver function generally normalizes within 1-4 months of stopping PN; but in some cases, prolonged liver dysfunction and even fibrosis has been reported(23). Several overlapping mechanisms may contribute to PN associated liver disease(24). These include prolonged duration of PN therapy, sepsis, low serum albumin, excessive caloric load, enteral fasting, nutritional deficiencies of taurine, choline, carnitine, phytosterol, manganese, oxidative stress and hormonal factors like elevated insulin/ glucagon ratio, gut hormones and biliary stasis. Simple interventions such as minimizing the duration of therapy, prevention and early detection and treatment of sepsis and choosing enteral over parenteral nutrition whenever possible, will minimize liver injury. Ursodeoxycholic acid (UDCA) is used in the therapy of cholestasis. It has been postulated that UDCA increases the hydrophilic non-hepatotoxic bile acid pool, decreases hepatocyte display of histocompatibility antigens and gives direct cytoprotection(25). UDCA is available as Tab Udiliv (300 mg) and the dose is 20-30 mg/kg /day. Electrolyte and trace element deficiencies Careful monitoring of fluid losses is essential to avoid electrolyte deficiencies. Most of the trace element deficiencies are due to improper supplementation and monitoring in long term TPN(26). Adequate levels of calcium may be hindered by incompatibility with other electrolytes, especially phosphorus. L-cysteine, which is present in the amino acid solution improves the solubility of both calcium and phosphorus. Catheter related complications These may be either technical or infectious in nature. Proper placement of the catheter with strict aseptic technique may reduce these complications. Peripherally inserted central catheters have a lower incidence of infection(19). Hematologic effects Thrombocytopenia, eosinophilia and hemolysis can occur following lipid administration. Thrombocytopenia and platelet dysfunction are believed to be dose related (30). Maximum lipid administration of 2-3 g/kg/day or temporary discontinuation of lipids would result in normal platelet count and function(14). Cost of TPN On an average, the cost of the TPN infusate with additives is around Rs. 700-800/day in our unit. Commercially available TPN solutions with prices are given in Table V. TABLE V Commercially available TPN Solutions in India
Cost saving should not be done by economizing on disposables, biochemical monitoring and infusion pumps. Laminar flow hood for mixing solutions is a must. Cost can be reduced by sharing the bottles between two patients, if two patients are receiving TPN at the same time. Transition to enteral feedings While parenteral nutrition provides the neonate with nutrients to sustain life and promote growth, its use can have negative physiologic effects on the gastrointestinal tract(22). Enteral starvation results in decreased secretion of gastrointestinal hormones, atrophy of gastric mucosa, decreased Immunoglobulin A production, a decline in gastrointestinal motility and an increase in the incidence of intestinal ulceration. These effects result in a decline in the digestive and absorptive capabilities of the GI tract and a loss of protective effects, increasing the risk for systemic bacterial infections. To minimize these effects, enteral feeding should be started as soon as possible. In our unit, we start small trophic feedings (small volume feeding given at the same rate for at least 5 days) as early as possible. For many neonates, parenteral nutrition is a life saving intervention, providing energy for growth and tissue repair when the gastrointestinal tract cannot be used. This is especially true for preterm and extremely low birth weight neonates. Familiarity with the nutritional requirements, complications and methods of monitoring parenteral nutrition will help minimize the risks to this population. Newer Perspectives Manganese The recognition that manganese is an essential trace element has led to its incorporation into parenteral solutions. A study in children on long term TPN showed increased signal intensity on T1 weighted images of the basal ganglia on MRI(27). Hence, manganese supplementation in neonates with long term PN needs further appraisal(28). Glutamine Glutamine supplementation has been recommended to prevent morbidity and mortality in preterm infants. The available data from good quality randomized controlled trials suggest that glutamine supplementation does not confer clinically significant benefits for preterm infants(29). Carnitine Carnitine is essential for the oxidation of long chain fatty acids. It is required to transport these fatty acids across the inner mitochondrial membrane to their site of oxidation with the mitochondrial matrix. The preterm has low plasma and tissue concentrations of carnitine and decreased capacity to synthesize carnitine, hence carnitine supplementation may have some role in ELBW infants on long term PN. Carnitine is available as injection Carnitor and the dose is 10 mg/kg/day. However, this issue needs to be confirmed by more studies(30). Lipid preparations Currently available lipid preparations contain triglycerides derived from soyabean oil and safflower oil. European trials are evaluating medium-chain triglyceride intra-venous lipid preparations(19). These may have an improved rate of oxidation, less chances of displacement of bilirubin from albumin and more carnitine content. Early initiation of enteral feeding There is no clear evidence to show that early initiation of enteral feeding in a parenterally fed ELBW infant is better than late initiation of enteral feeding according to the Cochrane database(31). Needless to say that there is plenty of evidence to show that enteral feeding is always preferred over parenteral nutrition, whenever possible. Among infants given trophic feeding, there was an overall reduction in days to full feeding and total hospital stay compared to infants given no enteral intake(32). In our unit, we start small trophic feeds as early as possible. Use of standardized versus individualized PN solutionsm Many centres abroad are now opting for standard or stock preparations than going through the laborious process of mixing the solutions. Yeung, et al. studied standardized versus individualized PN solutions for neonates <33 weeks gestation. They found no significant clinical and statistical differences in newborn infants in both the groups. However, the cost of PN went down by 30% when standardized solutions were used(33). These solutions are presently not available in India. Acknowledgement The authors are grateful to Dr. Umesh Vaidya for setting up TPN and establishing TPN protocols in our NICU.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()