|
|
Brief Reports Indian Pediatrics 2004; 41:1143-1147 |
||||||||||||||||||||||||||||||||||
|
Comparison of Improvement in Quality of Life Score with Objective Parameters of Pulmonary Function in Indian Asthmatic Children Receiving Inhaled Corticosteroid Therapy |
||||||||||||||||||||||||||||||||||
|
Meenu Singh, Joseph L. Mathew, Prabhjot Malhi, B.R. Srinivas and Lata Kumar From the Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh 160012, India.. Correspondence to: Dr. Meenu Singh, Additional
Professor, Department of Pediatrics, Manuscript received: November 27, 2003, Initial
review completed: January 23, 2004;
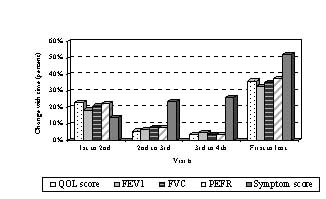
Key words: Asthma, Corticosteroid, Pulmonary function, Quality of life. Bronchial asthma impairs not only respiratory function, but also physical, social and emotional components of life. The severity of disease is usually assessed using clinical criteria and measuring objective pulmonary functions. Treatment initiation and modification are often based on evaluation of these parameters. While these criteria do provide subjective and objective assessment of clinical status, they require high level of patient motivation and cooperation, hence are often not feasible in younger children. Besides, the overall impact of the disease on the life of affected children cannot be estimated by these measurements. Children with similar symptoms and pulmonary function tests (PFT) may experience different levels of distress and dysfunction in their lives(1). Likewise, children on therapy may feel and function better than before, suggesting improved quality of life (QOL); but this positive change may not be reflected in conventional measurements. This study was, therefore, undertaken to compare changes in QOL score with objective measures of pulmonary function and subjective assessment of clinical status, in children with persistent bronchial asthma prescribed inhaled corticosteroid therapy. Subjects and Methods This prospective, hospital based, descriptive study was initiated after obtaining ethical clearance from the institutional Ethics Committee and children were enrolled with the written informed consent of parents/ guardians as well as assent of the children themselves. Twenty consecutive children in the age group eight to twelve years with newly diagnosed moderate or severe persistent asthma(2) were enrolled from the Pediatric outpatient department (OPD) or Asthma Clinic. Children with mental subnormality and those physically challenged were excluded. Children suffering from other chronic disease conditions involving respiratory system were also excluded. A detailed history covering personal history, family history, living conditions, known allergies and current as well as previous treatments was elicited at inclusion. Physical examination including anthro-pometric measurements was performed at the initial visit. During this visit, children and their parents were educated about the disease, therapeutic options, avoidance of triggers for acute attacks and familiarized with warning symptoms and signs of acute exacerbation. They were trained in the use of inhalation therapy, care and maintenance of inhalation devices and home monitoring of the child’s condition. They were each provided with a treatment plan and follow-up schedule. Children were also trained in the performance of spirometry and peak expiratory flow measurements. Children were administered the QOL questionnaire, underwent spirometry and measurement of PEFR with a Mini-Wright’s peak flow meter. The symptom diary used in the Asthma Clinic(3) was explained to the parents and they were instructed to fill it up daily. The QOL tool used was an indigenously developed, pre-tested, disease specific and culturally appropriate questionnaire for Indian children with bronchial asthma(4); it had been found to be a valid, reliable and reproducible tool(5). The questionnaire was developed in two language versions–English and Hindi; consisting of 41 points in 4 domains (21 for physical activity, 12 for symptoms, 4 for emotional functions and 4 for environmental stimuli). The choice of language rested with the children. The questionnaire was administered by a single trained interviewer not involved in prescribing therapy. At the initial interview, children were asked to identify the physical activities that they performed on a regular basis and these individualized activities were retained for each child throughout the study. The interviewer used children’s recall to evaluate the extent of impairment of QOL during the two weeks preceding the interview. Children were asked to choose responses from the four-point response option card; wherein each item could be scored from 1 to 4. At each of the subsequent visits, the QOL questionnaire was administered before spirometry, PEFR measurement and calculation of symptom score. Spirometry was performed by a trained technician using Compact Spirometer (Cat No 42.000, Vitalograph Limited, Buckingham England). Forced Expiratory Volume in first second (FEV1) and Forced Vital Capacity (FVC) were recorded according to the recommendations of American Thoracic Society(6). PEFR was measured by Mini Wright’s Peak Flow Meter (Mini Wright Cat No 3103001, England) and percentage calculated against the expected/ predicted as per Indian norms(7). Symptom score was calculated from the symptom diary maintained by parent(s) over the preceding 7 days and consisting of 6 items to be scored viz., history of day time or night cough, wheezing, difficulty in breathing, missing of school, exercise intolerance and use of rescue medication. A score of zero was given for absence and 1 for presence of each of the items. Thus the weekly score could vary from 0 to 42. Adherence to prescribed therapy was evaluated by instructing the child to mark the dosage taken in a separate column on the symptom diary, and confirming the same with parents. The children were prescribed Budesonide 400µg per day for moderate and 800 µg per day for severe persistent asthma(8) in two divided doses, with a metered dose inhaler through a spacer. They were advised two inhalations of salbutamol (100 µg per actuation) with a metered dose inhaler through a spacer, as rescue medication whenever necessary. All children were instructed to attend hospital in the event of occurrence of pre-defined alarming symptoms. Three follow up visits were scheduled; the first was two weeks after the initial visit, the second two weeks later and the last four weeks after the third visit. At each visit, QOL questionnaire was administered, children were assessed clinically and underwent spirometry and PEFR measurement. The symptom diary during the preceding two weeks was reviewed and the score recorded. The mean and standard deviation of QOL score, FEV1, FVC, PEFR and symptom score was calculated for each visit and analysis of variance for repeated measures was used to compare data between visits, with p <0.05 taken as significant. The percentage change in each of the parameters between successive visits and the first and last visits was calculated. Results There were 11 males (55%) and 9 females (45%) with mean age 9.33 ± 1.24 years. The majority (85%) had moderate persistent asthma; as the number of children with severe persistent asthma was small, the results were not separately compared. Table I shows the QOL score, FEV1, FVC, PEFR and Symptom score at each visit. There was a significant change in each parameter compared to the preceding visit. Fig.1 shows the comparative change in each parameter between successive visits and first versus last visit. Table I QOL Score, pulmonary functions tests and symptom score at initial and follow up visits.
* p <0.01 for parameters between successive visits. **p <0.05 for parameters between successive visits.
Discussion This study has shown that there is significant improvement in pulmonary functions, symptom score and QOL score after initiating ICS therapy in children with persistent asthma. This reflects treatment related improvement not only in the target organ, but in overall functional status and subjective feelings as well. Conventionally, objective measures of pulmonary function are used to evaluate progress; although there is no gold standard tool to assess this. Measurement of pulmonary functions requires high degree of patient cooperation and also reasonably good pulmonary reserve to perform the tests. Therefore, interpretation of these objective measures is often hampered by subjective factors, particularly in younger children. Besides, the readings reflect a one-time measurement of the child’s status unless recorded serially, which is often not feasible in home-based care. Assessment of quality of life is able to overcome several of these limitations, since it provides information of the overall status over a longer duration. There are a few tools available in Western countries for evaluating QOL in asthmatic children(9,10); however they cannot be directly extrapolated to Indian children due to socio-cultural differences and behavioral/ life-style variations. One of the strengths of our study is the use of an indigenously developed, pre-tested, locally appropriate, disease specific tool for assessing quality of life. This study has shown that improvement in QOL score with treatment compares well with improvement in objective measures of pulmonary function. This indirectly indicates the efficacy of QOL score for measurement of clinical status. Although temporal changes in PFT compare well with changes in QOL score, absolute measurements during a particular visit may not have a strong correlation. This happens because QOL score evaluates the child’s condition over a longer time frame; in contrast, PFTs are a one-time measurement and reflect the child’s condition at the time of testing, which may not always be representative of the overall clinical status. Secondly, the PFTs are dependent on the effort and cooperation of the child. QOL and symptom score are less demanding on the child, and likely to reflect his/her functional status better. Thus the measurement of QOL and PFT complement each other for the evaluation of clinical status; the former reflecting control of asthma over the preceding period and the latter the status at the time of measurement. Therefore it is prudent to incorporate QOL measurement as a routine tool to assess asthma control. It will be useful to study whether therapeutic modifications can be made on the basis of changes in QOL score. It may even be possible to define a composite clinical assessment parameter incorporating QOL score, symptom score and PFTs. In this study, improvement in symptom scores lagged behind improvement in QOL score and pulmonary functions, although the overall change was greater. This may be because, the scores were calculated from a diary maintained by parents, who may exercise caution in reporting improvement, unless it is noted consistently. This type of problem is likely to occur with all tools using proxy rather than self-reporting. To conclude, this study has shown that improvement in QOL score with treatment of asthma is comparable with objective measures of pulmonary function; with some advantages over the objective tests. It will be useful to complement pulmonary function tests with QOL scores to assess overall clinical status on a long-term basis. Contributors: MS designed the study, corrected the manuscript, supervised management of subjects and will act as guarantor. JLM analyzed the data and prepared the manuscript. PM contributed to evaluation of QOL score in subjects. BRS assisted in collection of part of the data. LK provided overall guidance in patient management. Funding: None. Competing interests: None.
| ||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||
|
![]()