|
|
Letters to the Editor Indian Pediatrics 2003; 40:1108-1109 |
|||
|
Homolateral Linear Morphea with Coarctation of Aorta |
|||
|
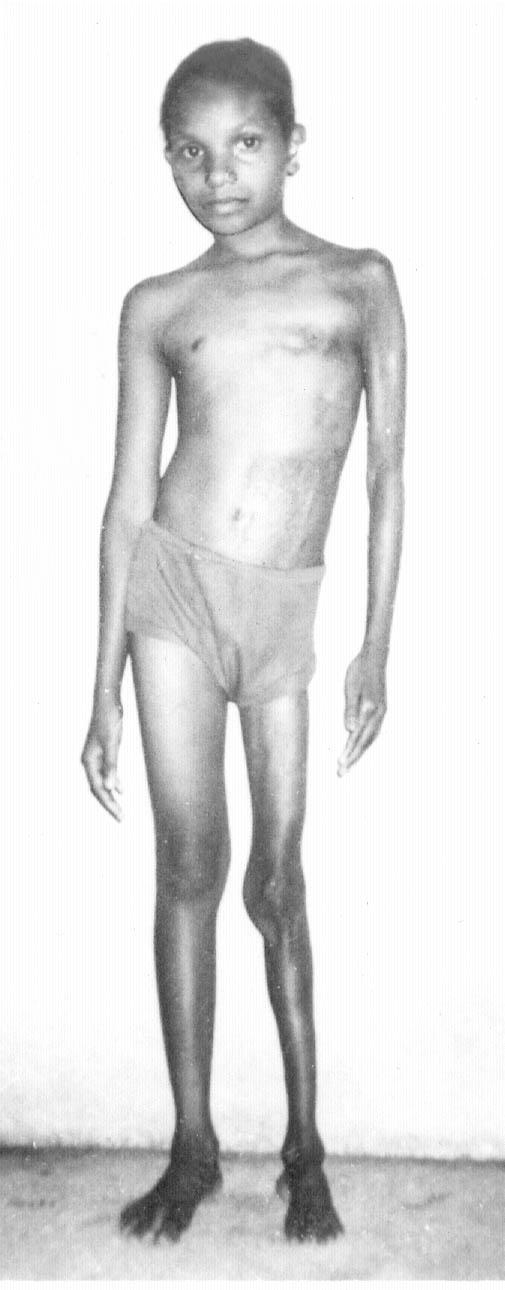
A 9-year-old female child presented with progressive atrophy of both left extremities and hyperpigmented patches over left half of the body since 3 years of age following a non-specific febrile illness. On examination, there was muscle wasting and true shortening in both the left limbs. Skin was fixed to the underlying bone. Multiple thick, indurated, hyperpigmented, hypoaesthetic, anhidrotic and depilated patches were present over left upper and lower extremities and left hemi-trunk sparing the head and face (Fig. 1). Talipes equinovarus and kyphoscoliosis were also present. She had no perioral skin fixation, esophageal dysmotility, arthralgia, myalgia, Raynaud’s phenomenon, respiratory or gastrointestinal symptoms. Motor power was grade III and deep tendon reflexes were absent on the left side. Left brachial and radial pulses were feeble. All pulsations were feeble in both lower limbs with radio femoral delay. Blood pressure was 140/100 mm Hg in right upper limb and non-recordable in both the lower limbs. She had absolute eosinophilia (1230/cumm) thrombocytopenia (60,000/cumm), positive antinuclear (ANA) and anti ds-DNA antibody. Rheumatoid factor was negative. X-ray of the affected limbs showed soft tissue calcifications. Abdominal ultrasonography and renal function tests were normal. Interestingly preductal aortic coarctation was seen in echo cardiography and colour doppler. Skin biopsy from a hyperpigmented patch over the abdomen showed thinning of the epidermis with loss of rete ridges, colla-genization of dermis with absence of pilosebaceous apparatus and subcutaneous fat without any eosinophilic infiltrate. The patient was treated with steroid, diphenylhydantoin and vitamin D3. No improvement in the platelet count or skin lesions was seen after 6 months.
According to the morphology and histo-pathology, it was a case of homolateral linear morphea. Non-exanthematous febrile illness was probably the precipitating factor. There was no known exposure to any drugs or chemicals. Kyphoscoliosis was secondary to limb shortening. Etiopathogenesis of morphea is immunological(2) supported by the presence of various autoantibodies. Of interest was the association of preductal coarctation of aorta. Coarctation is a congenirnl anomaly and is not related etiologically to morphea. Cardio-vascular pathologies associated with sclero-derma are myocardial fibrosis and ventricular hypertrophy(3). We think this association is very rare and not reported before in medical literature. Spontaneous recovery may occur with time in the milder form of the disease(4). The prognosis of the severe varieties is uncertain and remains guarded as definitive therapy is yet to be recommended. Sriparna Basu,
|
![]()