|
|
Letters to the Editor Indian Pediatrics 2003; 40:1105-1106 |
|||
|
Anhidrotic Ectodermal Dysplasia Presenting as Atrophic Rhinitis and Maggots |
|||
|
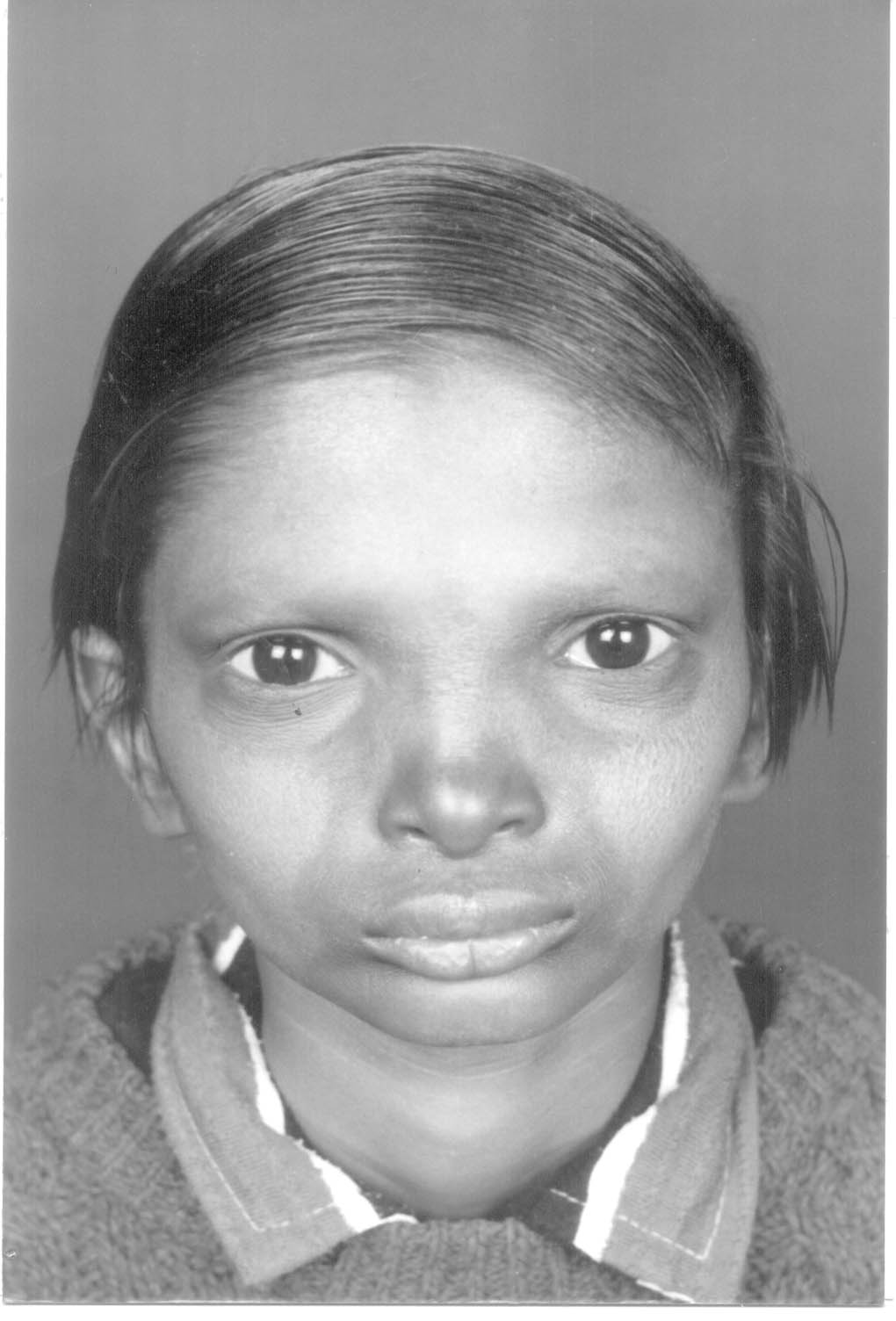
The first patient presented with complaints of occasional scanty epistaxis. On anterior rhinosocopy, he had all the features of atrophic rhinitis like wide roomy nasal cavity and crusts with maggots inside the nasal cavity. Patient also had typical features of anhidrotic ectodermal dysplasia like dry smooth skin with sparse blonde hair all over body. The facial appearance was also typical with depressed nasal bridge, prominent supraorbital ridges, dry protruding lips and fanning out of ear. Oral cavity showed high arched palate and defective dentition. The parents of the child and one elder brother were normal. There was no history of any still birth or abortion in the mother. The second patient was referred from the pediatric out-patient department for the complaints of epistaxis. He also had atrophic rhinitis with maggots inside the nose. The general appearance was ame as that of first patient; dry skin with blond sparse hair on head and eyebrows. He had no body hair and absence of perspiration. The skin of palm and sole was thick and rough with cellosities. The facial features were similar with supraorbital ridge prominence, depressed nasal bridge and protruding lips (Fig.1). Dentition was also abnormal. He had a younger male sibling with the same features but their parents were normal.
Anhidrotic ectodermal dysplasia is a sex linked recessive condition that manifests fully in affected males and partially in females(1). It’s association with atrophic rhinitis has been reported earlier even in infancy(2). The classical triad of anhidrotic ectodermal dysplasia consists of hypotrichosis, anodontia and anhidrosis. Ninety per cent of the affected patients are male. Absent or reduced sweating is a prominent feature. Biopsy confirms that eccrine glands are absent or rudimentary and this may be used as a basis for prenatal diagnosis. The facial features and apearance of these patients are conspicuous. Hypo-trichosis is generalized but incomplete with scraggly, thin, sparse, blond and dry hair. There is usually partial or total anodontia. Nails may be thin, brittle and ridged. The skin is soft, thin, dry and smooth. Mental retardation is present in some cases possibly as a consequence of hyperthermic episodes of childhood. The complete syndrome does not occur in females but carriers may show varying degree of dental defects, sparse hair, reduced sweating and dermatoglyphic abnormalities. Though the general appearance of the patient of anhidrotic ectodermal dysplasia is typical and hard to miss, it has to be differentiated from conditions like syphilis, leprosy which may present as secondary atrophic rhinitis with all its classical features of episatxix and not uncommonly maggots inside the nasal cavity. The local nasal condition has no permanent cure and nasal douching cures only the local nasal symptoms. The depressed nasal bridge occurs due to the compromised blood supply to the growing nasal and septal bones as a result of severe inflammatory reaction. Thus in any patient presenting with nasal maggots and occasional epistaxis and abnormal facial features, one should elicit the relevant history and make the necessary with clincial examination and investigations to rule out anhidrotic ectodermal dysplasia. V. Sinha,
|
![]()