|
|
Case Reports Indian Pediatrics 2001; 38: 1310-1314 |
||
|
Continuous Spikes and Wave During Slow Sleep |
||
|
Epilepsy with continuous spikes and waves during slow sleep (CSWS) is an uncommon type of epilepsy and is among the epilepsies classified as undetermined, whether focal or generalized. CSWS is a functional disorder of childhood with severe paroxysmal epileptiform discharges occupy-ing at least 85% of sleep (sleep index 85%). Seizures may be severe but self limited. Behavioral deterioration may occur with or without pre-morbid developmental abnor-mality, without any demonstrable brain pathology sufficient to explain the behavioral deterioration. Stabilization or improvement of behavior occurs, once the epileptiform EEG abnormality resolves(1,2). As an epileptic syndrome, CSWS can be considered transient and benign. Although patients experience severe epilepsy during CSWS, most seizures disappear spon-taneously before or near puberty(2,3). Nevertheless, the seriousness of this condition rests on the mental sequelae. Long term outcome with CSWS has been reported as poor in most patients. The outcome appears to be related to the age of onset and duration of the active phase of spike-and-wave discharge(2). Children with earliest and longest exposure to the active phase of continuous spike-and-wave discharge during sleep are at high risk for permanent sequel. Case Report A 6½-year-female child, full term vaginal delivery assisted by forceps with negative family history of seizures is being reported. There was no history of consanguinity in the parents. She had slightly delayed cry. In the immediate post-natal period she had 4-5 tonic-clonic seizures in a day which did not recur. Her developmental milestones were delayed – social smile at 3 months, neck holding at 5 months, sitting with support at 9 months and without support at 10 months, standing with support at 15 months and walking at 18 months. She could climb stairs at around 3 years of age. She started speaking monosyllables at 18 months and simple sentences (without verbs) at 3 yeas of age and there was no evidence of any focal neurological deficit. Vision and hearing was normal. She started going to school at 4 years of age, she could go up and down stairs, run and used to speak complete sentence using pronouns. At 6 years of age, she was noticed to have deterioration in her school performance and was also noticed to have absence seizures. EEG revealed 3 Hz spike and wave discharges. Following treatment with sodium valproate, the frequency of absences decreased significantly. But, 2-3 months later she started having complex partial seizures (CPS) and subsequnetly developed secondary generalization. Clobazam and carbamazepine were also tried before she consulted us. Her school performance continued to decline and gradually her word output decreased. She used to remain confused. All routine investigations including Computerized Tomography (CT scan) of head and Magnetic Resonance Imaging (MRI) of brain were normal. Awake EEG record, showed bilateral spike and wave discharges in the frequency of 2 to 3Hz and also showed some focal spikes predominantly in right frontal area (Fig. 1). While on the above mentioned three antiepileptic drugs, her seizure frequency decreased, but she became markedly confused and ultimately became nearly mute. Possibility of non-convulsive status epilepticus (NCSE) and CSWS was thought of and repeat EEG was advised. In spite of oral trichlorophos and intramuscular phenergan, the child could not be sedated and it was not possible to achieve sleep state. During the EEG recording, diazepam 5 mg was given slowly by intravenous route with the aim that EEG discharges might disappear if it would have been NCSE. However, EEG discharges got markedly exaggerated and whole of EEG record was almost completely occupied by generalized spike and wave discharges with frontal predominance (Fig. 1 right side). Though it was thought that the patient was suffering from CSWS, still 300 mg of Diphenylhydantoin (DPH) was given in 8-10 minutes to look for any response and subsidence of EEG discharges but the EEG discharges persisted to same extent. The possibility of CSWS became more obvious and the patient was started on Prednisolone 60 mg (2 mg/kg body weight) and continued for 6 weeks and was tapered in next 6 weeks. Carbamazepine and Clobazam were tapered slowly and Sodium Valproate dose was increased and continued. Clinically, she started improving. Her pre-treatment IQ was 90. Though post-treatment IQ was not done but clinically she became more alert and responsive and word output improved. Sleep EEG was repeated after 6 weeks. The EEG showed remarkable recovery and didn’t show any epileptiform discharges.
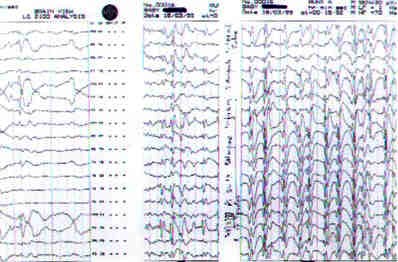
Fig. 1. The EEG records: Left side – Awake EEG record showing focal discharges predominantly in right frontal area. Middle Awake – EEG record showing bilateral spike and wave discharges with the frequency of 2–3 Hz. Right side – EEG record after diazepam and phenytoin: continuous generalized spike and wave discharges. Discussion CSWS is a rare disorder, the exact incidence of which is not known. Males are affected more commonly (63%) than females, the peak onset is usually between 5 and 7 years of age(3). Our patient had history of delayed developemental milestones. Prior abnormal neurological development is not uncommon in CSWS, and has been reported to be present in 31% of patients of CSWS. Seizures can be the presenting symptom in 80% of patients of CSWS. Our patient had onset with absence seizures. Subsequently she developed CPS with secondary generalization and aphasia and psychomotor retardation. The child was initially started on Carbamazepine and later on Sodium Valproate and Clobazam was added to control the seizures. Neuroimaging CT and MRI were normal. In CSWS, neuroimaging is usually reported to be normal in majority of the cases(3). Corticosteroids therapy, either with prednisone or ACTH appears to have favorable and long lasting effect(4,5). The patient improved with 6 weeks therapy of prednisone. EEG recordings in slow sleep are important for confirmation of the diagnosis of CSWS. During the active phase of spike and wave discharges most patients (78%) meet the criteria of a sleep index of 85% of EEG record shows epileptiform discharges). The average frequency of the spikes and waves is 2Hz. Sleep spindles may be absent. Patients could be divided into two groups, depending on the severity of the EEG abnormality. The first group has a sleep index of 85% or greater, frequently disrupted sleep spindles, only rare focal discharges during sleep, and bursts of spike and wave in wakefulness. This EEG pattern is seen in 70% of patients. The second group, shows a sleep index between 50% to 80%, often recognizable sleep spindles, more frequent focal spiking during sleep, and absent or rare spike and wave discharges during wakefulness. Focal spikes tend to be frontal. This EEG pattern is seen in 30% of CSWS patients. Landau-Kleffner syndrome (LKS) most closely resembles CSWS. LKS, also known as acquired epileptic aphasia (auditory agnosia), occurs in a previously normal child with normal language function and without a structural substrate. Continuous spikes and wave discharges during slow sleep are less than 85% of total record. Focal discharges tend to be centro-temporal or parietal in LKS and frontal in CSWS. Seizures in CSWS may be identical with those in "benign focal epilepsy with centro temporal spikes" (BECT) but sleep activation never reaches the 85% threshold required for the diagnosis of CSWS. In CSWS, focal abnormalities are predominant in the frontal areas, whereas in BECT they are maximal in the centro-temporal area. Family history is positive in 40% and 10%, respectively in BECT and CSWS. Atypical benign partial epilepsy of childhood is characterized by transiently severe epilepsy, but the apparently short duration of this condition separates it from CSWS(6). Lennox-Gastaut Syndrome (LGS) distinguishes itself from CSWS by specific EEG characteristics during sleep. Tonic seizures, runs of rapid rhythms and bursts of polyspikes and waves are not found in CSWS. In CSWS, the paroxysmal abnormality is restricted and time dependent whereas in the LGS the eileptiform activity is multifocal, persistent, and usually secondary to CNS injury. After giving diazepam, spike and wave discharges markedly increased in our patient. This may be used as a diagnostic tool. As the name suggests CSWS – discharges are during slow sleep. Diazepam induces slow sleep in few seconds and these discharges are known to increase during slow sleep. We propose that the diazepam induced slow sleep makes the epileptiform discharges very prominent, which are fairly suggestive of CSWS. In view of our experience with 11 patients of Non Convulsive Status Epilepticus (NCSE) complex partial seizures type, the commonest type of NCSE who were given diazepam on the table showed marked decrease of discharges or normalization of EEG (personal observations). However, a larger study is required to confirm the consistency of diazepam test in CSWS. If confirmed, it could be very simple, safe and cheap diagnostic tool to differentiate CSWS from NCSE, as in most of NCSE patients, diazepam is known to decrease or suppress epileptic discharges completely, while in CSWS it may worsen the epileptiform discharges. In suspected cases of CSWS where sleep EEG may be difficult to record or one needs to differentiate it from NCSE, EEG recording after diazepam should be done to diagnose CSWS and it may help to decide about appropriate therapeutic approach. Contributors: MMM diagnosed the case, interpreted and drafted the paper; he will act as the guarantor. JB and PA participated in data collection and drafting the paper. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()