|
|
Case Reports Indian Pediatrics 2001; 38: 1305-1309 |
||||||
|
Familial Fibrodysplasia Ossificans Progressiva: Trial with Etidronate Disodium |
||||||
|
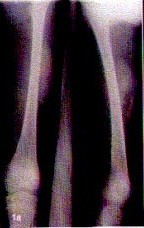
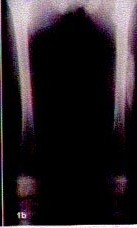
Fibrodysplasia or myositis ossificans progressiva (FOP) is a rare disorder of connective tissue characterized by congenital malformation of the great toe and by progressive heterotopic ossification of tendons, ligaments, fasciae and skeletal muscle occurring in predictable anatomic patterns(1). Frequently, the first sites of heterotopic bone formation occur within fibroproliferative lesions on the upper back and neck(1). Episodes of soft tissue swellings are usually spontaneous but may occur after minor trauma. The disease usually leads to extra-articular bony ankylosis of nearly all joints of axial and appendicular skeleton. FOP is thought to be transmitted as an autosomal dominant trait with variable expressivity; however, most cases are sporadic. There is no known effective therapy. Ethane-1 hydroxy-1 diphosphonate (Etidro-nate disodium) and Isotretinoin are the two drugs studied in the management of FOP(2-7). As very few families are reported in world literature (none from India), we describe here a father and a son suggesting an autosomal dominant mode of transmission treated with etidronate disodium. Case Report Case 1: The patient was the second child born out of nonconsanguinous marriage with uneventful birth and normal development. He presented with complaints of nodule forma-tion at site of intramuscular injection since 3 years of age, developing several days after injection. These nodules were not associated with any fever, redness of overlying skin or any tenderness. These nodules used to disappear spontaneously after 15 days to 1 month without leaving any persistent swelling. The patient also developed radial deviation of left wrist joint for last 6 months without any preceding trauma or swelling. A swelling also appeared in his right thigh a week after presentation to us without any obvious injury. Physical examination revealed a child with normal intelligence, no deafness, radial deviation of left hand with proximally placed thumb, normal phalanges and no clinodactyly. There was, however, no deformity of big toe. Hypotonia and bulging of anterior abdominal wall on left side was also noted. A week later, a non-tender swelling was noted in his right thigh without any redness of overlying skin but with restriction of movement. Skeletal survey revealed calcified plaques on anterior abdominal wall in periumbilical and right iliac fossa. On questioning, there was no history of abdominal injury. X-ray of the right thigh done a day after appearance of swelling was normal. When repeated after, 3 weeks along with Doppler studies, it revealed a large calcified mass lesion in mid thigh separate from the shaft of femur suggestive of myositis ossificans (Fig. 1a). Rest of the investigations including creatine phospho-kinase, electro-physiological stuides done to rule out muscle dystrophies were normal. The therapy regime included etidronate disodium orally in the dose of 20 mg/kg/day for 2 weeks followed by 10 weeks of treatment with 10 mg/kg/day with an interval of 12 weeks between courses. The child has received one course of 12 weeks followed by resting period of 12 weeks. During the course of treatment there were no further bouts of swellings and there was improvement in the ossification present in the right thigh (Fig. 1b). Laboratory examination at initiation and follow up period showed no abnormality in blood count, calcium/phosphorus levels, liver and renal functions. Case 2: The father of the index patient was 38 years old, who was symptomatic since the age of 3 years with the complaints of development of hard lumps over different parts of body appearing spontaneously or after minor trauma. Physical examination revealed palpable hard lumps over left upper arm and right big toe. Various deformities included ankylosis of left wrist in dorsiflexion and valgus position, right elbow ankylosed in extension, short thumbs with clinodactyly and right big toe ankylosed at distal inter-phalangeal and metatarsophalangeal joint. The big toe, however, was normal. He had normal intelligence without any deafness. Radiological examination revealed ossified lesions in the soft tissues of arm and thigh. Investigations including his creatine phophokinase, electrophysiological studies and renal and liver function tests were normal.
Discussion FOP is a rare condition; its prevalence is ~0.6/1 million live births(1). Reproductive fitness is low, and most cases appear to arise by spontaneous mutation(8). The molecular cause and pathogenesis of FOP remains unknown. Overexpression of bone morpho-genetic protein 4(BMP 4) in immortalized lymphoblastoid cells has recently been associated with this condition(9). However, BMP 4 expression is not elevated above normal levels in all cell lines patients with FOP, and mutations in the BMP 4 have not been identified in patients with FOP(9). In a study to identify the chromosomal location of the FOP gene, FOP phenotype was linked to markers located in the 4q27-31 region(9). Another study has localized the gene for FOP to chromosome 17q21-22(10). Heterotopic ossification in FOP is induced by minor injury to the soft tissue but can occur without detectable trauma. The pathological findings include perivascular lymphocytic infiltration into normal appearing skelectal muscle in the early phase followed by muscle cell degeneration and by highly vascular fibroproliferative soft tissue swelling that is indistinguishable histologically from aggres-sive juvenile fibromatosis. The fibroproli-ferative lesions evolve, through an endo-chondral process, into mature lamellar bone with marrow elements(9). Aggressive juve-nile fibromatosis can moreover be differ-entiated by absence of great toe abnor-malities. In children with previously affected members, it can often be recognized at birth or in early years before the onset of ossification because of the presence of shortening of the great toe (95%) and short thumbs (55%)(11). Early recognition allows protection of the child from injuries including avoidance of intramuscular injections or biopsy, wherein the damaged tissue serves as a focus of calcification. Our family had no abnormality of the great toe except a short thumb and clinodactyly in father and only proximally placed thumb in son without any shortening. Other family members did not reveal any skeletal abnormality. Deafness has been reported in almost 30% of case with FOP in a series of 42 cases suggesting its important implication in management of these children(11). None of our cases, however, had associated deafness. Biopsy of the lesion is not needed for diagnosis and is best avoided as it can form the nidus for an area of ectopic ossification. There is no known effective therapy for FOP. The benefits of therapy in this condition are also difficult to evaluate because the disease runs a long and very variable course. Objective assessment of the therapeutive agents is also difficult. Ethane-1 diphos-phonate has been tried due to its inhibitory effect on bone mineralization and its potential to impair the rapid ossification process observed after the acute episodes. The reports have been variable(2-5). In a case report on long term treatment with oral etidronate sodium, there were no typical bouts of swellings or hardening of areas over the skeletal muscle and there were no side effects. However, the disease gradually progressed leading to limitation of joint movement(5). Intravenous etidronate along with oral corticosteroid administration in 31 fibro-dysplasia ossificans progressive attacks showed rapid diminution of local inflamma-tion in 29 attacks. However, despite treatment with EHDP, 10 new ossifications were observed(6). Our patient received one course of etiodronate sodium with regression of ossification and no further flare-ups. It has been suggested that it is more effective during the initial period of treatment with a gradual decline in effectiveness later(5). Further follow-up is thus indicated to elucidate the long-term effect of the drug. Retinoids are another plausible family of therapeutic agents for FOP due to their ability to inhibit differentiation of mesenchymal tissue into cartilage and bone. In a study to assess the efficacy of isotretinoin, it decreased the incidence of heterotopic bone formation at uninvolved anatomic regions compared with an external control group, as long as the medication was started before the appearance of ossification in that region. The above study, however, did not determine the effect in preventing disease flare-ups suggesting extreme caution to be exercised while using this medication(7). Other agents used with-out success include adrenocorticotropic hormone, corticosteroids, dietary calcium binders, intravenous infusion of EDTA and warfarin(5). The severe disability produced by this disease merits early recognition so that good general care and avoidance of trauma (particularly iatrogenic trauma from intra-muscular injections, biopsies, and surgery) may be emphasized. Despite the equivocal benefit of treatment with EHDP, our patient demonstrated the possible inhibitory effect on the acute stage progression of the disease; however, the long term outcome is awaited. Contributors: VK, TD and MK were involved in collection of data and drafting the manuscript. VK will act as guarantor for the paper. Funding: None. Competing interests: None stated.
| ||||||
| References | ||||||
|
![]()