|
|
Case Reports Indian Pediatrics 2001; 38: 1301-1305 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Distal Renal Tubular Acidosis with Severe Bony Deformities and Multiple Fractures |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
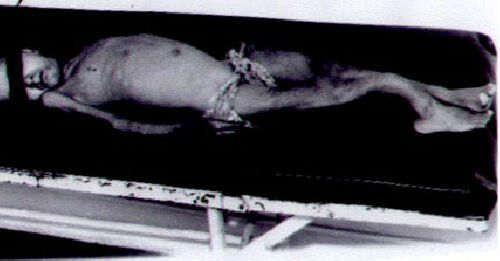
Distal renal tubular acidosis (RTA) is characterized by impaired hydrogen ion secretion resulting in metabolic acidosis with inappropriately alkaline urine(1). While bony deformities and rickets are reported, their severity is milder compared to proximal RTA(1). Multiple fractures have, to our knowledge, not been previously reported in patients with distal RTA. We report a 12-year-old child with severe bony deformities and multiple fractures secondary to distal RTA. The patient responded clinically, biochemically and radiologically to alkali supplements. Her 1-year-old sister also showed features of the same condition though of milder severity. Case Report This 12-year-old girl presented with severe and progressive bony deformities and multiple fractures. She was a product of a third degree consanguineous marriage, born at term by a normal vaginal delivery. There was history of pain in the extremities and bony deformities since early childhood. Multiple fractures occurred after trivial trauma. She had earlier been diagnosed as osteogenesis imperfecta (for recurrent pathological fractures) and hypophosphatasia (for persistently low normal alkaline phosphatase levels). There was history of polyuria and polydipsia since early childhood. There were no features suggestive of liver disease, malabsorption, parental neglect or willful injury. The child weighed 12 kg with a height of 107 cm, which were below the third percentile for age. There was widening of wrists, prominent costochondral junctions and bony deformities in the form of anterior bowing of tibia, curved forearm bones and ulnar deviation of the hands (Fig. 1). The patient was severely incapacitated due to the deformities and was non-ambulatory. Sclerae were normal in color; vision and hearing were within normal limits. Biochemical findings on blood and urine examination are summarized in Table I. The skeletal survey showed generalized osteo-penia, multiple loosers’ zones and healed fractures (Fig. 2). Ultrasound and CT scan of the abdomen showed bilateral nephro-calcinosis and nephrolithiasis (Fig. 3). The tubular maximum of phosphate/GFR was reduced at 2.1 mg/dl and generalized amino-aciduria was present. Serum albumin level was 3.8 g/dl. In view of hyperchloremic metabolic acidosis with normal anion gap, elevated urine pH, positive urine net charge, normal fractional excretion of bicarbonate, low urinary to plasma CO2 difference and hypercalciuria the patient was diagnosed to have distal RTA. Alkali treatment (Polycitra, 2 mEq/kg of bicarbonate/day) was started. Ten days later blood pH was 7.36, potassium 4.2 mEq/L, bicarbonate 23 mEq/L and alkaline phosphatase 650 IU/L. Treatment with chlorthiazide (2 mg/kg/day) was started for hypercalciuria. On follow-up one year later, she gained 5 kg weight and 4 cm height. The levels of blood pH, bicarbonate and potassium and urinary calcium were within normal limits. On this occasion, her one-year-old sister was brought to medical attention with polyuria and polydipsia. She showed failure to thrive with length and weight below the third percentile. Investigations showed hyperchloremic metabolic acidosis, high urinary pH, positive urinary net charge and low urinary to plasma CO2 difference (Table I). There was no evidence of rickets on skeletal survey. Ultrasound abdomen showed features of nephrocalcinosis in both kidneys. She was diagnosed to have distal RTA and treatment with alkali supplements was given.
Fig. 1. Photograph showing severe bony deformities in upper and lower limbs.
* At one year
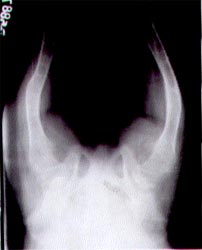
Fig. 2. X-ray hip (AP view) showing osteopenia, Loosers’ zones and healed fractures.
Fig. 3. Plain CT scan abdomen showing bilateral nephrocalcinosis. Discussion Patients with distal RTA usually present with failure to thrive, polyuria, polydipsia and acidotic breathing. Hyperchloremic meta-bolic acidosis with alkaline urinary pH is characteristics(1). Reduced ammonia produc-tion is an important feature of distal RTA. This is reflected by a positive urinary net charge, which is the sum of urinary sodium and potassium, minus chloride. Following bicarbonate loading the difference between urinary and blood CO2 is low(2). Hypo-kalemia, hypercalciuria and near normal alkaline phosphatase levels are associated with the condition. The diagnosis of distal RTA, in the present patient, was made on these findings. Distal RTA is inherited most commonly in an autosomal dominant manner. However autosomal recessive and X linked inheritance have also been reported. Presence of disease in these siblings and normal parents indicates an autosomal recessive inheritance in this family. Distal RTA may also be secondary to inherited diseases like hereditary fructose intolerance, galactosemia, hereditary ellipto-cytosis, sickle cell anemia and Ehler-Danlos syndrome(1). Severe osteopenia and bony deformities, which were seen in this patient, have rarely been reported in patients with distal RTA. Bone disease in distal RTA has classically been described as mild osteopenia, while frank rickets is uncommon(3). Rickets is more commonly reported in patients with proximal RTA(3). The cause of rickets in patients with distal RTA is not clear. It has been suggested that chronic metabolic acidosis may affect vitamin D metabolism. Rachitic deformities resolve following alkali supplementation and treatment with vitamin D is not required(4). Blood levels of vitamin D metabolities have however, been found to be normal in these patients(5). Increased urinary losses of calcium has been proposed to cause hypocalcemia and secondary hyperparathyroidism in patients with distal RTA(6,7). Secondary hyperpara-thyroidism results in hypophosphatemia, reduced tubular maximum of phosphate and generalized aminoaciduria as in this patient(7). It is possible that the combination of hypocalcemia and hypophosphatemia may result in rickets in these patients. In a case series of 28 patients with distal RTA, 4 were found to have rickets. Patients with rickets had similar age at diagnosis compared to those without rickets(8). The former, however, showed evidence of vitamin D deficiency with low blood levels of 25-hydroxy vitamin D3. The authors suggested that metabolic acidosis may act as an aggravating factor to vitamin D deficiency. The present patient had distal RTA with severe bony deformities and fractures. Multiple fractures in patients with rickets, have been reported in preterm neonates with rickets of prematurity(9), vitamin D deficiency(10) and vitamin D dependent rickets(11). Severe bony deformities and multiple fractures in our patient might be attributed to delayed diagnosis with severe metabolic acidosis, hypocalcemia and hyper-parathyoidism. A low dietary intake of calcium and phosphorus, which is common in Indian children might also be contribu-tory(12). The latter might explain the severe bony deformities in this patient and the greater incidence of bony deformities in Indian children with distal RTA. Patients with distal RTA require alkali supplementation(1). The dose of bicarbonate required is usually 2-3 mEq/kg/day. Correction of metabolic acidosis reverses most biochemical abnormalities and bony changes of distal RTA. Vitamin D meta-bolites are not required and can be potentially dangerous as hypercalciuria is already present(5). In patients with persistent hyper calciuria treatment with thiazide diuretics and salt restriction is advised. Contributors: ABaj, SG, AS and AB were involved with the management of the patient. ABaj drafted the manuscript. AB reviewed the manuscript and will act as its guarantor. Funding: None. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()