|
|
Personal Practice Indian Pediatrics 2001; 38: 1252-1264 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Japanese Encephalitis |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Japanese encephalitis (JE) is a leading cause of viral encephalitis in Asia that has been controlled effectively through national vaccination programs in several countries like Japan, Korea, China and Thailand(1-3). It is endemo-epidemic in some regions in India(4,5). It is difficult to eradicate JE because it is transmitted from natural reservoirs like pigs and wading birds (herons and egrets)(3). In many Asian Countries, the disease burden due to JE remains unclear(1). Hospital based surveillance in Malaysia revealed JE to be responsible for 38.5% of hospitalized cases of encephalitis and 0.4% of non-specific febrile illnesses(6). Many epidemics have occurred in India since 1955(2,4). JE has been reported from 24 states/Union Territories in India so far(7,8). However, comparison of reported cases and expected cases from India indicates JE surveillance gap (difference between expected and reported cases)(1,9). Since JE deaths are always reported, but only 2% of JE cases are reported(1), Case Fatality Rate apparently increase proportionately. The case Fatality Rate (CFR) and morbidity due to JE can be reduced significantly by early diagnosis and appropriate supportive treatment(10-12). Epidemiology JE is the only virus so far confirmed to cause epidemics of encephalitis in India (other viruses cause sporadic cases)(10,13). JE has high mortality (20-50%)(13-15) and morbidity rates (0.3-1.5/10000 popula-tion)(16,17). The usually affected age group is 5-10 years though children from 1-15 years can also be afflicted(18). Boys are more frequently affected than girls probably due to dressing and playing habits(19). Adults may be affected either due to fresh introduction of virus (as in West Bengal) or vaccination of pediatric population(20). The Afganistan war is likely to affect the migratory birds especially Herons coming to India from Siberia. The trend of number of JE cases after 10th October (after the onset of war on 7-10-2001) reported in India may give us a hint regarding the role of these migratory birds in the causation of epidemics of JE in India. Virus Japanese encephalitis is caused by a zoonotic flavivirus. The North Indian strain of Japanese encephalitis virus (JEV) is GP78, which is phylogenetically closer to the Chinese SA14 isolate. The other, the Vellore P20778 isolate, was obtained from southern India in 1958(21). JE virus has a complex life cycle(2). In nature, JE virus is maintained in animals and birds, particularly pigs and Ardied birds (e.g., Cattle egrets, pond herons, etc.) Frogs, Snakes, Egrets, Bats and most domestic animals like cattle, poultry, ducks are also infected by the virus(5). Pigs and Ardied birds are the reservoir and amplified hosts and are unaffected by the infection. Horses and donkeys also suffer from Japanese encephalitis. Reservoir Pigs are the most important biological ampifiers and reservoirs(3). Countries that do not rear pigs like Pakistan had JE only very rarely(22). JE virus is carried by female mosquitoes from infected pigs(23,24) or water birds to susceptible children. Vector The main vector, Culex mosquito (Culex tritaeniorhynchus, C. vishnui, C. pseudo-vishnui and others–totally 11 species) breeds in flooded rice fields, marshes, and standing water around planted fields and can fly up to 5 kms. It rests on rank vegetation or sugarcane. This is the reason JE is mostly a rural disease. The spread of JE to new areas is probably due to agricultural development, intensive rice cultivation and increased use of nitro-genous fertilizer(25), supported by irrigation schemes(26,27). Season Epidemics coincide with the monsoon and post monsoon period (August to December)(4). Drying of rice fields resulting in fewer vector habitats, lower temperature, and/or reduction of number of susceptible host animals may be resulting in termination of epidemics(28). However, in endemic areas, sporadic cases may occur throughout the year due to congenial climatic conditions (e.g., southern India). After mosquito bite, the disease appears in 5 to 16 days. The ratio of overt disease to unapparent infection varies from 1:270 to 1:1000(29). JE does not spread from child to child because of the low and transient viremia. Thus man is the accidental, dead-end host. Pathogenesis Primary multiplication occurs in extra-neural local sites, probably in fibroblasts. Virus then reaches the regional lymph nodes. Efferent lymphatics carry the virus through the thoracic duct to the blood stream. If the immunological response is adequate, as happens in the majority, the infection is either subclinical or mild. In susceptible individuals, the virus then invades the central nervous system probably by passive movement across cerebral capillaries or replication and growth across the capillary endothelium(30). Initially, brain damage is due to viral infection and multiplication in neurons per se, but later immunopathological mechanisms may play a role, as happens in many other CNS infections. Pathology Usually gray matter is involved. Lesions are seen in thalami, substantia nigra, cerebral cortex, cerebellum, Ammon’s horn, and anterior horn of spinal cord(31,32). Clinical Features Japanese encephalitis virus infection results in nonspecific symptoms necessitating laboratory studies in an individual case (10,14,33). The clinical manifestations depend upon three variables, namely, severity of infection, susceptibility of the host and location of the agent. The symptoms and signs of encephalitis may be enumerated under the following five headings:
Convalescence stage: There is defer-vescence of fever and neurologic improve-ment. The frequency of common symptoms and signs reported in various Indian studies are shown in Table I.
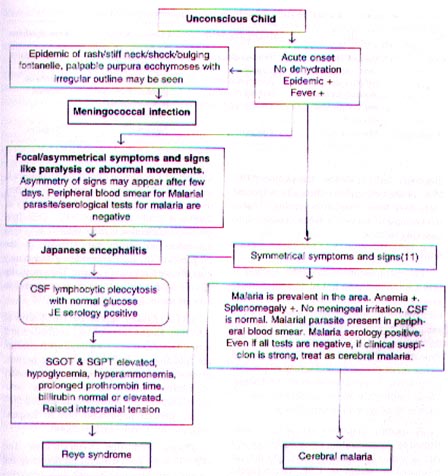
* Rathi et al. did not analyze focal/asymmetrical presentation. From the data presented, retrospective analysis revealed this figure (hemi or mono limb paresis 41.5, aphasia 36.2). Focality or asymmetry of tone, reflex, cranial nerve paresis and seizures were not mentioned. N = Focal/asymmetry of posture, tone, reflexes, cranial nerve or limb paralysis, seizures, movement disorders. +, 0 = Please note that movement disorders also indicate focal damage to basal ganglia and so have to be added to the cases having focal signs. Since, there is a possibility that other focal signs might have occurred in the same patients with extrapyramidal signs, it is not a simple addition of percentages, in the series of Kumar et al.(14) and Rathi et al.(33). Acute flaccid paralysis (AFP) has been reported in JE(35,36). So serology for JE is desirable in all cases of AFP(37). These clinical findings are nospecific and mean different diagnostic possibilities during an epidemic and during sporadic case presen-tation. A high suspicion at the beginning of the monsoon/rainy season is the only way to avoid missing the diagnosis of JE. The diagnosis at the primary health center (PHC) level is based on clinical symptoms only. Therefore, there is a need to develop simple tests for use at the peripheral level both for diagnosis and for epidemiological surveys(16). A flow chart (Fig. 1) has proved useful in this context in Andhra Pradesh(10). CSF Analysis The clinical suspicion of encephalitis can be supported with CSF analysis (Table II). Neutrophils are seen in early few hours of acute phase and lymphocytes after the first few hours. Lymphocytic pleocytosis (usually 10 to 60 lymphocytes/mL {complete range 6 to 1000 lymphocytes/mL} occurs with normal glucose level.
Fig. 1. Suggested Clinical approach during epidemics of Coma in India for field use(10).
Serological Tests A serology report requires more than a week and so this test is not useful immediately for the management of a critically ill patient(38,39). Serology, therefore, is useful only for retrospective confirmation of diagnosis and epidemic management(10). Most of the times, many clinically suspected cases may have a negative serology (Table III) because of various reasons in addition to sampling methods.
Antibody detection The recommended diagnostic method is IgM capture enzyme linked immunosorbent assay (ELISA)(42). There is no cross reactivity with other antigens when ELISA is used(43). Specific IgM antibodies can be detected in CSF, serum or both in approximately 75% of the patients by the 3rd day of onset of disease and nearly all patients are postivie 7 days after onset of the disease. These antibodies are detectable for one to three months after the acute episode. A specific diagnosis can also be con-firmed by demonstrating a four fold or greater rise in serum IgG antibody titer. IgG may be estimated in serum or CSF. Heterologous flaviviral antibodies, e.g., to dengue and West Nile viruses are a potential source of false positive reactions(44-46). Important Points About Serodiagnosis Sero-confirmation is desirable in the initial phase of an outbreak and in sporadic cases. In outbreak situations, it is neither required nor is it feasible for laboratory to confirm all the cases. Only a representative number of samples to clinch the diagnosis is sufficient(10). During epidemics, depending on the sample and method, the sensitivity of diagnosis could be up to 90%. CSF IgM antibodies detection is more reliable than IgM antibodies in serum for arriving at the diagnosis of JE, since antibodies in blood may not indicate CNS involvement. The sensitivity of CSF IgM is about 80-90% as compared to 10% of serum IgM(17,47). IgG antibodies appear by 10-14 days of infection. Rising titers of IgG antibodies in 2 serum samples taken 7-14 days apart confirm the infection. If IgG antibodies are present, estimation of IgM antibodies is necessary to confirm recent infection, since sero-prevalence of IgG antibody can exceed 50% in the general population due to frequent exposure to JE virus earlier(20,48). Plaque Reduction Neutralization Test (PRNT) is the gold standard for detecting and quantifying Japanese encephalitis neutraliz-ing antibodies. This test takes about a week and is carried out in 6 or 24-well plates, which limits its usage for large-scale screening. A simplified assay has been developed recently(49). Detection of viral genome by polymerase chain reaction is easier to perform and highly reliable(7,8) with 100% sensitivity but is expensive(50). Method of sending samples for serology At least 5 ml blood is drawn, kept at room temperature for 30 minutes (for blood to clot) and then kept at 4º C in the refrigerator for 30 minutes (for the clot to retract). The serum is then separated and sent in a cold chain after labelling with a period for serological testing. Demonstration/isolation of virus/antigen from CSF/brain, though ideal not only for the JE virus but also for any variants of the virus or detection of a new virus, is still not feasible on a large scale. Neuroimaging Findings are nonspecific and may be caused by many viral infections. These findings reflect edema of affected areas as nonenhancing hypodensity on CT and prolongation of T1 and T2 relaxation times on MRI. MRI is superior to CT scan of brain. Cranial MRI reveals either mixed intensity or hypo intense lesion on T1 and hyper intense or mixed intensity lesion on T2 in thalami. Thalamic changes may be helpful in the diagnosis of JE especially in endemic areas(51,52). Hemorrhagic transformations have also been described in JE lesions, with corresponding expected T1 and T2 changes. SPECT shows hypoperfusion in thalamus, frontal cortex and lentiform area consistent with the crucial role of thalamus and its connections in the genesis of movement disorders in JE(53). The substantia nigra is also involved in Japanese encephalitis(54).
Differential Diagnosis During epidemics, cerebral malaria, Reye’s syndrome and meningococcal infec-tion must be considered as other important possibilities (Fig. 1 and Table II). When there is no epidemic, these CSF changes (increased pressure, normal glucose, lymphocytosis and elevated proteins in CSF) may suggest one of the following: other viral meningitis or encephalitis, partially treated bacterial menin-gitis, parameningeal infections, tuberculous or fungal meningitis in the early phase, parasitic infections (e.g., toxoplasmosis, tri-chinosis), postinfectious encephalomyelitis, or active demyelinating disease. Management There is no specific treatment for JE. No effective anti-viral drugs are available. The principles of management of comatose children must be followed in general(10,55). The main reason for the high morbidity and mortality rates in India is either delay or improper/inadequate nursing care(10,39). Only 1 death out of every 6 deaths is directly due to JE virus and 5 out of 6 are preventable with prompt and early management bringing down the case fatality rate of JE from 35-50% to less than 6%. A similar degree of lowering of morbidity is also possible. Management includes prevention and treatment of complications like aspiration, status epilepticus, raised intracranial tension, hypoglycemia, hyperpyrexia, airway block, severe hypotension, syndrome of inappro-priate ADH secretion, secondary infections, pulmonary edema, stress ulcers and preven-tion of corneal injury. The basic principles of management include:
Recurrence of JE Recurrence of symptoms after apparent recovery with fresh neurologic deficits or mortality can occur. The virus remains latent in peripheral lymphocytes, and can later cause recrudescence(57). Prognosis Japanese encephalitis represents a severe disease in children with a high early mortality. Mortality was significantly related to a short prodromal stage, deep coma, abnormalities in tone and breathing and decerebrate posturing(14). In another study, acute JE at younger age, with higher body temperature, high white cell count in CSF, and deep coma present at hospital admission were markers for unfavorable outcomes (sequlae or fatal)(15). Sequelae of the disease were more severe when the initial illness was prolonged or was associated with focal neurologic deficits(58). A tumor necrosis factor (TNF) concentration over 50 pg/mL in serum correlated significantly with a fatal outcome, whereas high levels of JE virus IgM antibodies (more than 500 units) in the CSF were associated with a nonfatal outcome(59). Short-term studies of Post JE disability demostrated neurologic sequelae in 25%-75% of survivors(16,18,58,60,61). Reduced IQ was reported among 32% of JE survivors(62). Markedly severe dystonia is an important and serious sequela of Japanese encephalitis and may occur as the result of thalamus, midbrain, or basal ganglia involvement in various combinations(63). Most of the sequelae continue to improve over years. In general, those neurological functions which have a large area of representation in the cortex (like cortical motor deficit, memory loss, intellec-tual deficits, speech abnormalities) are affected very frequently and so occur in a large number of patients in the initial phase but recover to a great extent since the unaffected neurons in that part of the cortex take over the function in contrast to those neurological functions which have a small area of representation like substantia nigra, which occur in fewer patients but have very small chance of recovery. This is because of complete damage to small collections of neurons (like substantia nigra resulting in Parkinsonism, cranial nerve nuclei resulting in cranial paralysis) with sparing of insufficient number of neurons to take over the lost function and compensate. Long Term Therapeutic Measures Drug Therapy, physiotherapy and rehabilitation measures are necessary for sur-vivors with sequelae like seizures, paralysis, psychiatric problems(64), movement dis-orders, incontinence and Parkinsonism. Long Term Preventive Measures Measures to control mosquitoes, shifting pigsties, environmental sanitation (prevents many other diseases also), avoiding mosquito bites (prevents many other diseases also), and vaccination of the susceptible population (best of all measures) are useful. Vaccine China, Korea, Japan, Taiwan and Thai-land faced major epidemics of JE in the past but controlled it primarily with vaccina-tion(1). The only internationally licensed JE vaccine, an inactivated mouse-brain derived vaccine, is efficacious but is problematic from the perspectives of reactogenicity, require-ment for numerous doses, cost and reliance on a neurolgocial tissue substrate. Protective immunity induced by the inactivated JE vaccine includes JE virus-specific T cells as well as antibodies with multiple biological activities. Mouse brain-drived, Beijing-1 and Nakayama JE vaccines induce high levels of neutralizing antibodies. High levels of induced antibodies are maintained at least for 3-4 years. Administration: For children above 3 years and adults, two doses of 1 ml each (0.5 ml for children under the age of 3 years) should be administered subcutaneously at an interval of 7-14 days. A booster injection of 1 ml should be given after 4 weeks to 1 year in order to develop full protection. Revaccina-tion may be given once after 3 years in endemic areas. Immunization is supplement-ed by booster effect of natural JE infection in endemic areas. So JE incidence has declined in countries with national programs of routine JE vaccination (Japan, Korea, Thailand and China). Those residing in non-endemic zone need further periodic vaccine boosters every 3 years. Desirable age group for vaccination is 2 to 15 years. The induced antibodies are cross-reactive to heterologous strains. Indian JE vaccine is a Formalin inactivated vaccine made from the brain of suckling mice inoculated with the Nakayama JE strain, produced at the Central Research Institute (CRI), Kasauli, Himachal Pradesh. As there is no man-to-man transmission and man is a dead end for the virus, vaccination (unlike polio) protects only the vaccinated and does not protect the commu-nity at large. A single dose of JE vaccine produces immunity within a week in only 50% and if the child develops JE because of a natural infection, it is likely to be attributed to JE vaccine. This limits its use for control of epidemics and so must be used during inter-epidemic periods. Unless 80-90% of children less than 15 years are vaccinated, there will not be any obvious effect on morbidity and mortality in the community. Reactions to vaccine Side effects are generally limited to mild local effects. Generalized symptoms are rare (e.g. fever is seen in only 5%). Most of these side effects are transient. Newer vaccines (available in China, not yet available in India) Attenuated SA14-14-2 single dose Japanese encephalitis (JE) vaccine has been adminsitered safely and effectively to more than 100 million children in China since 1988 and Korea(65). It is safe for children and effective with one dose costing about Rs. 20/- However, production and regulatory standards are unresolved(1). Co-administration of JE Vaccine with other Vaccines Simultaneous and nonsimultaneous vaccination with MMR, poliomyelitis, hepatitis A, hepatitis B, diphtheria, tetanus, yellow fever, typhoid fever or rabies vaccines results in similar immunogenicity for JE virus. JE Vaccination in India In endemic areas, where sporadic cases occur throughout the year, the cost effectiveness of vaccination is very low to be considered as the method of choice. To protect infants in hyperendemic districts, 18 million doses of JE vaccine (costing Rs. 60 crores for vaccines + operational costs) are required and this has to be followed by boosters every 3 years, which has enormous cost and operational implications. Since the risk of JE is not universal and is limited to focal areas, JE immunization is not included in the National Immunization program in India and it is recommended for active immunization only in JE prone areas. There is a need for a proper pilot trial on JE vaccination involving 3-4 hyperendemic districts for making a policy on mass JE vaccination in the community. In conclusion with proper health education, early diagnosis and treatment, and environmental sanitation, we can also control this recurring national health problem as has been done by countries like South Korea, China and Japan. Acknowledgement The Director of Health, Government of Andhra Pradesh has opened 100 special encephalitis wards all over the state of Andhra Pradesh in various Government Hospitals. The data supplied by the Directorate of Health, Andhra Pradesh were analyzed and used partly for the preparation of this article. The interested reader is referred to the detailed latest version with step by step description at the website: http://www.ind med.delhi.nic.in and http://www.gist.ap.nic. in/articles/health Funding: Part of this article reflects the work done in wards created during epidemics of Japanese Encephalitis in Government Hospitals of Andhra Pradesh. The facilities like beds, medical and nursing care, follow up in outpatient, and drugs were provided by Director of Health, Government of Andhra Pradesh. The author has not received any specific funding for the work. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()