|
|
Brief Reports Indian Pediatrics 2000;37: 1234-1238. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Profile of Pediatric Malignancies: A Ten Year Study |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Rojimon Jacob Rema Jothirmayi M.K. Nair
Malignant neoplasms are rare in children. Its impact on children’s lives varies with its incidence, diagnosis, therapy, mortality and survival at different places and times. Childhood cancers are unique in the sense that they arise from embryonal cells, respond to treatment rapidly and the survival has improved dramatically over the last two decades due to aggressive combined modality management(1,2). Improvements in survival have also been shown to be associated with increased centralization of management. Cancer is an important cause of mortality in many of the economically developed nations of the world. More than 10% of all deaths in children below 15 years of age are caused by malignant diseases in developed countries. In the developing world, childhood cancers are yet to be recognized as a major pediatric illness due to several other competing causes of death like diarrheal illness and respiratory illness. However, due to considerable reduction in infant and child mortality rates experienced in a few developing countries, it is emerging as a distinct entity to be dealt upon. For instance the infant and child mortality rates in Kerala are considerably below national average and in tune with the increase in the diagnosis of degenerative diseases, childhood cancers are being increasingly diagnosed(3). An attempt is made in this paper to describe the pattern of pediatric cancer seen at Regional Cancer Center, Thiruvananthapuram, which is likely to more often reflect the pattern in the community. In the absence of reliable population registration, hospital statistics in developing countries provide the only available window to observe the disease pattern in the community.
All cases of malignant disease in children registered between January 1983 and December 1992 were included in the study. The case records pertaining to the age group 0-14 years were analyzed to find out the descriptive clinical profile of these patients. Benign intracranial neoplasms, histiocytosis - X and connective tissue tumors of borderline malignancy were also included. Histological diagnosis was confirmed by our pathologist in all cases except for surgically inaccessible intracranial tumors. Histological classification system used was the one proposed by Birch and Marden(4).
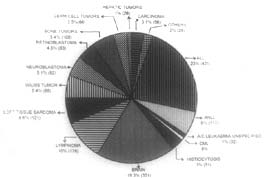
Total number of patients registered during this 10 years period was 1828 and accounts for 4.5% of all cases registered in this center. Figure 1 shows the distribution of cases according to the classification scheme recommended by Birch and Marden(4). The commonest malignancy was acute leukemia accounting for 30% of all cancers. Acute lymphoblastic leukemia (ALL) represented the commonest form of malignancy (23%). Acute myeloid leukaemia (AML) was seen in 6.4% of all cases (ALL: AML - 3.6: 1). A few cases were grouped as acute unspecified leukemias because of the diagnostic difficulties encountered. The diagnosis was based on morphology and cytochemistry. Lymphomas were seen in about 10% of cases of which non-Hodgkin’s lymphoma (NHL) was more common (6.6%). Most of the NHLs were high grade and diffuse. The most common histological subtype of Hodgkins disease was mixed cellularity.
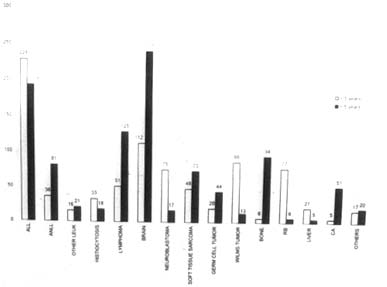
Fig. 1. Relative frequency of tumor types in children 0-4 years of age. Intracranial and other Central Nervous System tumors were the largest group of solid tumors in childhood. Common tumors were astrocytomas, gliomas and medulloblastomas. Embryonal tumors like neuroblastoma, retino-blastoma, Wilms’ tumor and hepatoblastoma were more common in children under the age of 5 years (Fig. 2). Osteosarcoma (OS) and Ewings sarcoma (ES) were the two common forms of bone tumor of which osteosarcoma was slightly more common. Rhabdomyo-sarcoma was the most common histological subtype seen among soft tissue sarcomas. Of the germ cell tumors, majority (81%) were arising from gonads. Carcinomas were rare and seen in about 3% of cases; nasopharynx, thyroid and salivary glands were the common sites. In general, the malignancies were more in males and 46% of all cancers were seen in children below 5 years of age.
Fig. 2. Frequency of tumor types in children below the age of 5 years. Relative Frequencies (%) of Different Forms of Pediatric Malignancy in Present Series and Four Developed Countries
Childhood tumors form a highly specific group, mainly embryonal in type and arising in the lymphoreticular tissue, CNS, connective tissue and viscera, epithelial tumors are rare. Classifying cancer by anatomic site is satisfactory for cancers in adults, but it is not suitable for classifying cancer in children. It does not reveal frequency of one type of cancer. Hence, the classification scheme used was according to the recommendation of Birch and Marsden(4). The general pattern of pediatric tumors in our center seems to resemble the distribution of pediatric cancers reported from other countries (5-10). Leukemia was the leading type of cancer and malignant tumors of CNS were the second most common cancer in childhood in several countries. The same finding was noted in our series also. Acute leukemias were the most common type of childhood cancer in our series and 75% of all leukemias were ALL. Incidence of ALL was more in the age group 1-4 years in both sexes. The relative frequency of different forms of pediatric malignancy in our series in comparison to developed countries is shown in Table I. Marked differences were found in the age distribution of various cancers. The frequency of ALL, neuroblastoma, Wilm’s tumor, retinoblastoma and hepatoblastoma were strikingly more in children younger than 5 years of age. An increased frequency with age was seen in non-Hodgkin’s lymphoma, Hodgkin disease, osteosarcoma and Ewings sarcoma. The early onset and the embryonal nature of many pediatric tumors suggest a prenatal origin. Male predominance is a salient feature of many childhood tumors. Sex ratio also varies with site. The male excess is particularly marked in neoplasms of lymphoid origin i.e., in ALL, NHL and HD which represent over one-third of all tumors. Environmental factors like exposure to carcinogens at work or smoking habits may be contributing to excess of cancer in adult males, but such an explanation cannot account for the excess of cases seen in male children. Genetic difference in immune function may be responsible for the increased incidence of lymphoid tumors in males. The female excess seen in germ cell tumors may be due to earlier development of ovarian tumors than testicular tumors, but no convincing explanation is given for increased incidence of sacrococcygeal teratomas in girls. There are reports of geographic differences in the incidence and frequency of cancer in children. Data available from population based cancer registries at Bangalore, Bombay and Madras show that 3.7 to 4% of all cancers is constituted by pediatric neoplasms(11). In Dibrugarh in the north eastern India and Chandigarh in the north western India the frequency was 2% and 4.8% respectively(12). The proportion of childhood cancers seems to be high compared to that of developed countries where there is a lower proportion of children in the population. The international comparison of cancer frequency and incidence are potentially biased by variability in diagnosis, classification and differential access to medical care and incomplete registration and hence has to be interpreted with caution. The number and relative proportion of various histological subtypes referred to a treatment center may not reflect their distribution in the population. At present we have no population based statistical data on childhood cancer. It is, therefore, not possible to assess the magnitude of the cancer problem in our country according to standard statistical methods. Accurate incidence of data are important in the planning and evaluation of clinical trials. Establishment of committed pediatric cancer registries in India will certainly contribute to useful clinical epidemiological research. Contributors: KP co-ordinated the study and drafted the paper; she will act as the guarantor. RJ and RJ were responsible for data collection and analysis, MKN guided the study. Funding: Nil.
|
![]()