Even with dedicated neonatal intensive care
facilities, most of the Indian tertiary care centers lack specialized
cardiac care facilities and surgical back-up. Many neonates with
duct-dependent circulation, despite being on prostaglandin infusion,
require adequate mixing at the atrial level for adequate oxygenation.
Many such neonates are not stable enough to be transported. Urgent
balloon atrial septostomy at the referring center is the only bail-out
option in many of these neonates.
With many neonatal units being equipped with in-house
echocardiography facility, with basic training of point-of-care
echocardiography and easily accessible hardware (which can be sterilized
and reused in resource-limited settings), this procedure can be done
bedside by a cardiologist adequately trained in the procedure. The need
of the procedure should be decided by neonatologist in consultation with
cardiologist.
 |
|
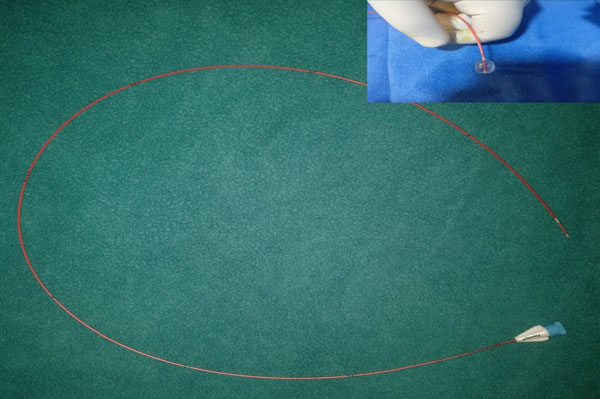
Fig. 1 Fogarty’s (4F) arterial embolectomy catheter,
its tip has a balloon which has to be inflated during the
procedure.
|
Here in we describe the steps, hardware needed and
special precautions to be taken for this procedure. After obtaining
consent, venous access is obtained via femoral or umbilical
route, and a 4F/5F pediatric sheath is exchanged over the guide wire.
Fogarty’s catheter (Fig. 1) is passed under
echocardiography guidance from inferior vena cava (IVC) to right atrium
and probed in to patent foramen ovale (PFO), and is guided in to left
atrium. Once in to left atrium, the balloon is inflated with saline and
position confirmed on echocardiogram. With a rapid controlled jerk of
balloon, membranous inferior margin of the foramen ovale is torn
allowing good flow across PFO (Web Video 1).
Controlled jerk is necessary to avoid any injury to IVC. We emphasize
that proper training under expert guidance/supervision is required
before one attempts this procedure.


