An 8-year-old boy presented to us with daily, multiple seizures for the
last 6 months. The parents reported brief jerking of limbs lasting for
few seconds resulting in occasional falls. These episodes had been
treated elsewhere as generalized tonic-clonic seizures with phenytoin
and carbamazepine, with no response. There were no other seizure types
or any history of cognitive decline. The family history was
unremarkable. Clinical examination, and magnetic resonance imaging (MRI)
of the brain were unremarkable and video-EEG is shown (Fig. 1
and Web Video 1). The clinico-EEG features were
consistent with a diagnosis of idiopathic epilepsy with myoclonic
absences (MAE). His karyotype was normal. The seizures stopped after 2
months on valproate and clobazam.
 |
 |
|
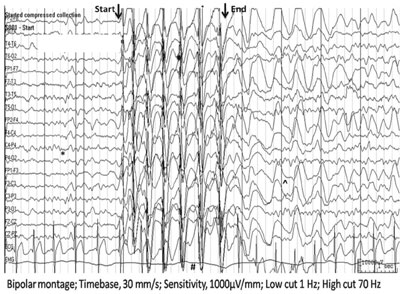
Fig. 1 and Web Video 1 Abrupt onset
and offset of rhythmic, repetitive and bilateral myoclonic jerks
involving shoulder, arms and legs associated with uprolling of
eyeballs and period of unresponsiveness that lasts for 3 sec in
Video 1. Onset of this brief clinical event was time-locked with
generalized, high amplitude 3 Hz spike wave discharges (#) that
lasted for 3 seconds till the end of clinical event followed by
frontocentral delta slowing(^) (Fig. 1). This burst of
generalized discharges was preceded by normal 8-9 Hz posterior
dominant awake EEG rhythm (*) (Fig. 1).
|
MAE is very rare epileptic syndrome and the classical
semiology consists of brief, bilateral myoclonic-jerks involving
shoulders, arms and legs (time-locked with EEG-discharges), with
variable impairment in consciousness with abrupt onset and termination.
The predominant tonic contraction of shoulder muscles result in the
classical elevation of the arms. Co-occurrence of the other seizure
types is unusual in idiopathic subtype.
These repetitive myoclonic jerks are often mistaken
for rhythmic clonic jerks. Presence of multiple such episodes in a day
of brief duration with period of unresponsiveness and immediate recovery
to normalcy along with ictal EEG correlate of 3 Hz suggests myoclonic
absence seizure rather than generalized clonic seizures. Such seizure
semiology may be seen in a neurologically normal child; but more
commonly, it is seen in a neurologically abnormal child who may have
abnormal EEG, abnormal neuroimaging or chromosomal abnormalities.
The treatment requires high-doses of valproate with
lamotrigine or ethosuximide. However, the seizures may be resistant to
treatment.


