|
|
|
Indian Pediatr 2015;52: 441 |
 |
The False Positivity of Positron Emission
Tomography Owing to Teething
|
|
Erman Atas and Vural Kesik
Gulhane Military Medical Academy, Department of
Pediatric Oncology, Ankara, Turkey.
Email: [email protected]
|
|
In cancer treatment, diagnostic tools and treatment options have
improved tremendously. However, the results of diagnostic tests
sometimes may not be compatible with clinical course, and cause a
dilemma whether the patient is in remission or relapse.
A 13-year-old-boy with T-cell lymphoblastic lymphoma
was treated with chemotherapy (BFM-NHL-95). The patient was in remission
after evaluation of protocol I Phase I. After protocol I phase II, all
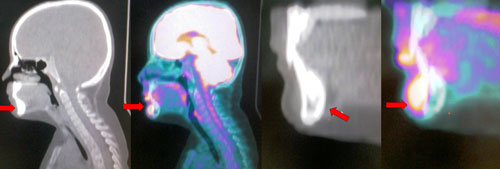
parts of body were normal except pathological 2-fluoro-2deoxy-D-glucose
( 18F-FDG) uptake of mentum
anterior (SUVmax: 14.9) (Fig. 1). On physical examination,
teething was seen in this region. The uptake was attributed to teething,
and treatment was continued with protocol M. After this protocol,
pathological FDG uptake was not detected in any part of body. The
patient is in good condition with no tumor recurrence in the maintenance
treatment.
 |
|
Fig. 1 FDG uptake on the mentum
anterior (SUVmax:14.9).
|
Positron emission tomography (PET/CT) imaging can be
used as an excellent tool in the diagnosis, staging and restaging of
cancer. A glucose analog, 18F-FDG,
is taken up by cells via glucose transporter, which then undergoes
phosphorylation by hexokinase to FDG-6 phosphate. This does not undergo
further metabolism and becomes trapped in the cells with high metabolic
rate – in malignant tumors pathologically, and some normal tissues
physiologically [1]. Response criteria are updated in adult lymphoma to
include PET/CT, but its utility is under investigation in the pediatric
lymphomas [2,3]. It is unclear whether the abnormal findings in PET/CT
are enough to change therapy [4] because false positives and false
negatives are possible on PET/CT. Physiologic 18
F-FDG uptake in lymphoid tissue, brown adipose
tissue, glandular tissue, muscular system, gastrointestinal tract, and
inflammation due to radiation, chemotherapy, trauma or infection are
some of the causes of false positive interpretations [5].
Acknowledgments: Dr Ceren Yildirim and Dr Ozgur
Karacalioglu for providing clinical and technical support on the
evaluation of this patient.
References
1. Pauwels EK, Ribeiro MJ, Stoot JH, McCready VR,
Bourguignon M, Maziere B. FDG accumulation and tumor biology. Nucl
MedBiol. 1998;25:317-22.
2. Cheson BD, Pfistner B, Juweid ME, Gascoyne RD,
Specht L, Horning SJ, et al. Revised response criteria for
malignant lymphoma. J Clin Oncol. 2007;25: 579-86.
3. Bakhshi S, Radhakrishnan V, Sharma P, Kumar R,
Thulkar S, Vishnubhatla S, et al. Pediatric nonlymphoblastic
non-Hodgkin lymphoma: Baseline, interim, and posttreatment PET/CT versus
contrast-enhanced CT for evaluation-A prospective study. Radiology.
2012;262:956-68.
4. Cheng G, Servaes S, Zhuang H. Value of (18)
F-fluoro-2-deoxy-D-glucose positron emission tomography/computed
tomography scan versus diagnostic contrast computed tomography in
initial staging of pediatric patients with lymphoma. Leuk Lymphoma.
2013;54:737-42.
5. Long NM, Smith CS. Causes and imaging features of
false positives and false negatives on 18F-FDG /CT in oncologic imaging.
Insights Imaging. 2011;2:679-98.
|
|
|
 |
|
