|
|
|
Indian Pediatr 2015;52: 440 |
 |
Aneurysm of Right Branch of Portal Vein in a
Child
|
|
*KP Srikanth and BR Thapa
Division of Pediatric Gastroenterology, Department of
Gastroenterology, PGIMER, Chandigarh, India.
Email: [email protected]
|
|
Portal vein aneurysm (PVA) is a rare congenital or acquired abnormality
of the portal circulation which constitutes for about 3% of reported
venous aneurysms in children and adults [1]. In majority of the cases,
they are asymptomatic, and are detected incidentally on imaging of the
abdomen. Only few cases of PVAs have been reported in children. We
evaluated a 12-year-old girl for intermittent abdominal pain. She did
not have history of abdominal trauma or major illness in past. Hemogram,
liver function tests and renal functions, including urine microscopy
were normal. As a part of routine investigation, she underwent
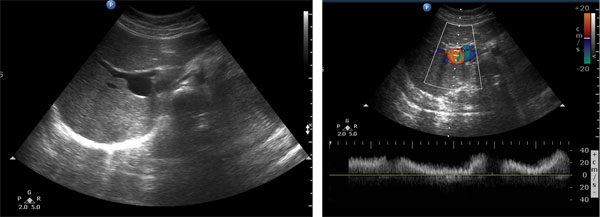
ultrasonography of abdomen which showed an anechoic structure along the
course of right branch of portal vein (Fig. 1a). On color
doppler, the lesion showed color fill with venous waveform pattern on
spectral analysis (Fig. 1b) suggestive of venous aneurysm
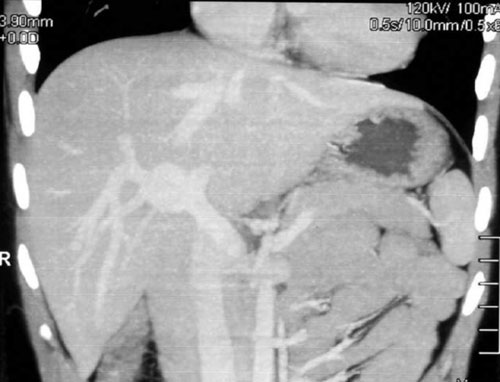
which was confirmed by dual phase computed tomography (CT) study (Fig.
2). Upper gastroentestinal endoscopy, done to rule out portal
hypertension, was normal. Child was managed conservatively, and pain
subsided after two weeks without any intervention.
 |
|
Fig. 1 (a) Transverse gray scale
ultrasound image of liver showing anechoic lesion arising from
right branch of portal vein (b) venous waveform on pattern
spectral waveform analysis.
|
 |
|
Fig. 2 Coronal reconstructed CT image
of venous phase showing saccular aneurysm arising from right
branch of portal vein.
|
PVA is a fusiform or saccular focal dilation of the
portal venous system which was first described in an adult by Barzilai
and Kleckner in 1956 [2]. The maximum dimension of the normal portal
vein is upto 15 mm in normal individuals and 19 mm in case of cirrhosis.
Thus the upper limit considered for labeling as portal vein aneurysm is
taken above 20 mm as there is considerable variation in the size across
different age groups [3,4]. Usually the dilatation of the portal veins
occurs in the setting of hepatocellular disease and portal hypertension
due to various etiologies. Congenital venous aneurysms occur without any
predisposing conditions because of underlying weakness along the course
of vein, and can be associated with anomalies of other organs. Color
Doppler ultrasonography is considered to be the gold standard for the
diagnosis of the venous system anomalies together with CT or Magnetic
resonance angiography. The complications are spontaneous rupture into
the bile ducts resulting in hemobilia, thrombosis, and obstruction
leading to porto-systemic shunts [2]. Smaller and asymptomatic lesions
are left without any intervention, and the larger ones need angiographic
coiling or surgical aneurysmorrhapy. To summarize, congenital PVAs are
rare, usually asymptomatic, and can be managed conservatively.
Acknowledgments: Dr Akshay Saxena, Dr Sadhna
B Lal, Dr Anmol Bhatia and Dr Babu Lal Meena for helping in management
of this case.
References
1. Molinares B, Alvarez S, Garcia V, Sepúlveda ME, Yepes
NL, Peláez S. Extrahepatic portal vein aneurysm after liver
transplantation in a child: Case report. Pediatr Transplant.
2013;17:E33-6.
2. Barzilai R, Kleckner M. Hemocholecyst following
ruptured aneurysm of portal vein; Report of a case. AMA Arch Surg.
1956;72:725-7.
3. Doust BD, Pearce JD. Gray-scale ultrasonic
properties of the normal and inflamed pancreas. Radiology.
1976;120:653-7.
4. Lee HC, Yang YC, Shih SL, Chiang HJ. Aneurysmal
dilatation of the portal vein. J Pediatr Gastroenterol Nutr.
1989;8:387-9.
|
|
|
 |
|
