An 8-month-old boy presented with high grade fever of 7 days
duration and few reddish lesions on face, scalp and upper
limbs (Fig. 1). To start with, there were few
lesions on the face that gradually increased in size and
number to attain the present status. Drug history, past
history and family history were non-contributory except for
common cold and mild fever about 10 day prior to onset of
cutaneous lesions. Cutaneous examination revealed multiple
well-circumscribed erythematous to violaceous papulo-nodules
and plaques (few targetoid) over the face, scalp and both
upper extremities. Hairs, nails, and mucosa were unaffected;
conjunctivae were congested. Laboratory investigations
revealed leukocytosis with neutrophilia and raised
erythrocyte sedimentation rate. Punch biopsy followed by
histopathological examination of a representative lesion
from face showed dense perivascular neutrophilic infiltrate
along with vasodilatation, nuclear dust and upper dermal
edema, without any evidence of vasculitis. A diagnosis of
acute febrile neutrophilic dermatosis was made, and
prednisolone (1mg/kg/d suspension) was started under
antiobiotic cover. Lesions showed improvement at the end of
1st week of treatment.
 |
|
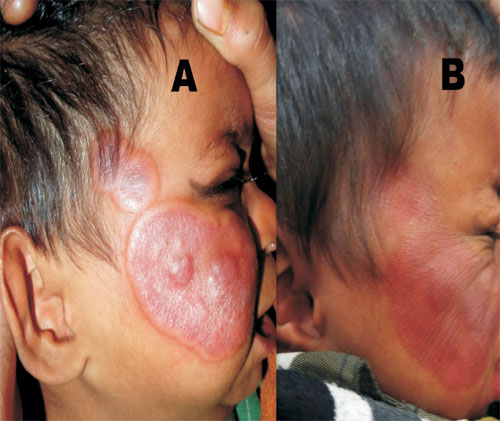
Fig. 1 Well defined
erythematosus to violaceous plaques and nodules on
face (A) and flattening of lesions (B) after one
week of treatment.
|
Acute febrile neutrophilic dermatosis,
also termed Sweet syndrome (SS), is a reactive process
characterized by the abrupt onset of tender, red-to-purple
papules, and nodules that coalesce to form plaques. The
plaques usually occur on the upper extremities, face, or
neck and are typically accompanied by fever and peripheral
neutrophilia. SS may be idiopathic or may be associated with
infections, inflammatory conditions, malignancy pregnancy,
or drugs. Clinical differentials include erythema nodosum
leprosum in leprosy patients (presence of features
suggestive of leprosy); cellulitis or erysipelas (mostly
single lesion, boil prior to the onset of lesion); erythema
multiforme (preceding drug history or infection, presence of
target lesions); urticaria (transient, itchy) and leukemia
cutis. The criteria for diagnosis have been proposed by Su
and Liu, and revised by Driesch.
The treatment options include systemic
steroids saturated solution of potassium iodide, dapsone and
clofazimine, besides treatment of the underlying condition.


