|
|
Letters to the Editor Indian Pediatrics 2006; 43:456-457 |
|||
|
Gradenigo’s Syndrome |
|||
|
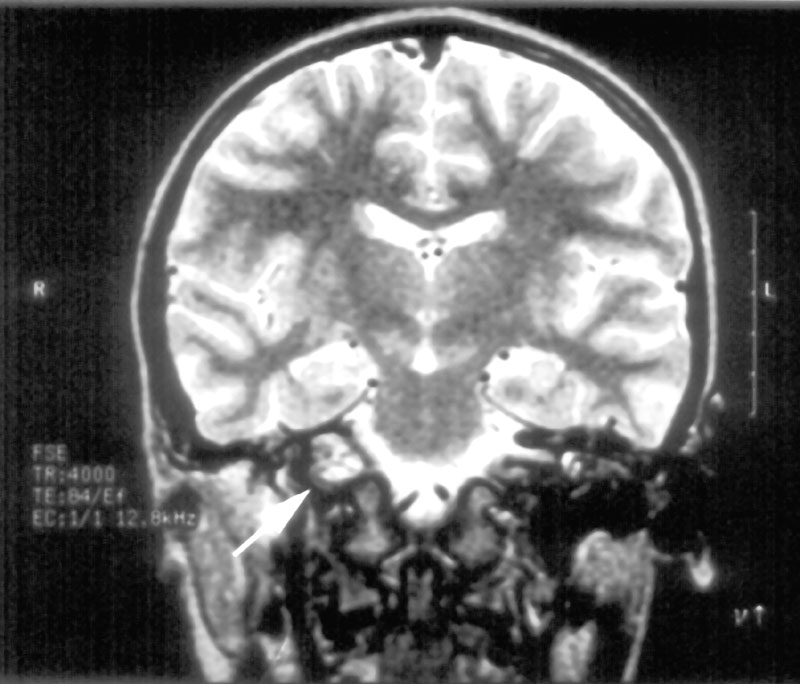
A nine-year-old girl presented to hospital with pyrexia (39.3ºC), photophobia, diplopia, discharging ears and a right lateral rectus palsy. The child’s mother was treating the child with homeopathic medicines instead of the antibiotics prescribed by her doctor for otitis media. Examination revealed bilateral otorrhoea with perforated ear drums, redness and swelling of the right eye, with normal visual acuity. There was tenderness over right side of her face, neck and mastoid region along with enlarged cervical lymph glands. Her white cell count was 14.4 × 109/L, (neutrophilia - 81%) and C Reactive Protein was 173 mg/mL (normal <10). Ear swab grew b-hemolytic Group A streptococci. Blood cultures were sterile. CT scan of head showed left ethmoid and sphenoid sinusitis, opaci-fication of both maxillary antrum and mastoid air cells, and soft tissue densities in both middle ears extending to the attic. No bony destruction or focal brain abnormality was seen. MRI revealed inflammation of the petrous apex that was not evident on CT (Fig. 1).
She was treated with broad-spectrum antibiotic and patching of the eyes. Complete resolution was noted after 2 months. Gradenigo syndrome consists of 3 components: otitis media, pain in the distribution of the 1st and 2nd divisions of trigeminal nerve (V cranial nerve) and ipsilateral abducent nerve (VI cranial) paralysis. The trigeminal nerve ganglion and the abducent nerve lie adjacent to the apex of the petrous bone(3-4). Osteitis and local leptomeningitis near the apex of the petrous bone can cause the cranial nerve dys-function(5). Occasionally the facial nerve (VII cranial) can be affected(3). Presentation may be with weakness of the lateral rectus and diplopia, accompanied by ocular and facial pain, photophobia, lacrimation, corneal hyperesthesia and often a deep-seated headache. Gradenigo’s syndrome can also arise due to extradural abscess or pachymeningitis overlying the petrous apex without petrositis per se(4). Phlebitis from the lateral sinus spreading along the inferior petrosal sinus can also produce this(4). Acknowledgements The authors thank Dr. Farhad Aref-Adib, Consultant Radiologist, for help with the imaging. Jayanti J. Rangasami,
|
![]()