|
|
Letters to the Editor Indian Pediatrics 2006; 43:454-455 |
|||
|
Gelastic Epilepsy and Hypothalamic Hamartoma |
|||
|
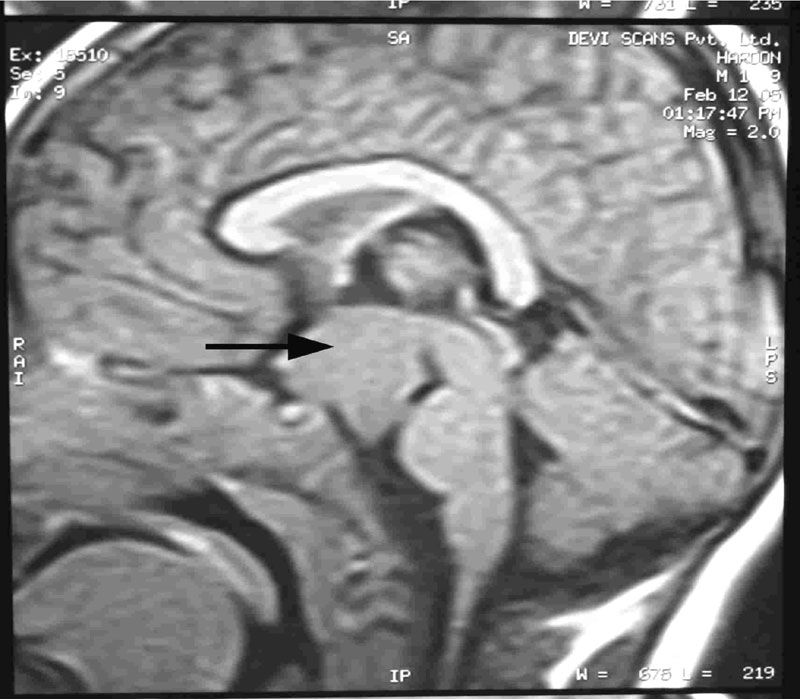
A 1½-year-old male child born out of non consanguineous marriage presented with progressively increasing episodes of unprovoked stereotyped laughter lasting for few seconds since the age of 5 months. Along with this, child was having excessive weight gain and signs of premature development of secondary sexual characters as hair growth in face, axilla and pubic area, with enlarged penis and large testis for his age. He was also having concomitant squint. There was no other neurological deficit. A clinical diagnosis of gelastic seizures with obesity and precocious puberty was made. MRI brain showed a lobulated isointense solid lesion on TIW and relatively hyper intense on T2W and FLAIR images noted in the region of hypothalamus between infundibular stalk and mamillary bodies with splaying of cerebral peduncle posteriorly measuring about 2.3 × 2.3 × 2.8 cm. The lesion did not enhance on post contrast study (Fig.1). The morphology is suggestive of hypothalamic hamartoma. Patient was started on sodium valproate and dose increased upto 1000 mgs per day and his seizure frequency was not reduced significantly. In view of gelastic seizures along with signs of hypothalamic endocrine dysfunction as obesity and precocious puberty patient was referred to neurosurgery for resection of hamartoma. Histopathology examination confirmed hypothalamic hamartoma and patient became seizure free for last six months with out antiepileptic medication.
Hypothalamic hamartoma is the most common structural cause of gelastic seizures (1). Gelastic seizures have also been described with cortical dysplasia in the cingulate gyrus(3). Hypothalamic hamartoma may be a part of Von Recklinghausen disease or polyostotic fibrous dysplasia, which is a leading cause of precocious puberty in both boys and girls. Crying and sobbing seizures may alternate with gelastic spells in the same patient(2,5). Some patients only have interior feeling of pressure to laugh without overt manifestations(5). Hypothalamic hamartoma often cause executive function disorders. Rarely it can cause excessive secretion of GnRH that cause early onset androgen secretion and spermatogenesis in boys and estrogen secretion and cyclic ovarian secretion in girls(1). This leads to premature development of secondary sexual characters leading to precocious puberty. Obesity is not a well-recognized feature associated with hypo-thalamic hamartoma(1,2). MRI usually shows a collar button like lesion typically lying between the infundibular stalk and mamillary bodies. The lesion does not enhance but is slightly hyperintense to gray matter on T2 weighted study(1,4). The immediate differential diagnosis is a hypothalamic glioma that usually enhances strongly and uniformly following contrast(5). The Gelastic seizures may respond to anticonvulsant like sodium valporate. Majority of the patients had good out come after partial resection(1). Here our patient had Gelastic seizures resistant to anticonvulsants and he underwent resection of hamartoma and remained seizure free thereafter. S. Syamlal,
|
![]()