|
|
Letters to the Editor Indian Pediatrics 2004; 41:518-519 |
|||
|
Bedside Clue to Bilateral Partial Nasal Obstruction in a Neonate |
|||
|
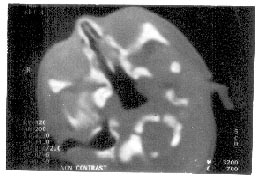
A term neonate weighing 2800 grams was delivered by normal vaginal delivery and cried immediately after birth. He had respiratory distress but normal chest on clinical and radiological examination. Nasal flaring was absent. Bilateral choanal obstruction was suspected. The diagnosis was confirmed by failure to negotiate an 8 Fr catheter through the nose and CECT (Fig. 1). ENT surgeons confirmed the diagnosis by endoscopy and ruled out bony atresia of the choanae. Following endo-scopy and decongestion the neonate stabi-lized and was discharged on the 10th day.
Various modalities, which suggest and confirm the diagnosis of bilateral nasal compromise have appeared in literature. Cyclic cyanosis has been described as the classic presentation whereby the respiratory distress in a an obligate nose breather is alleviated by crying. Absence of alae nasi activation in the presence of chest retraction has been poorly emphasized and often missed in common practice. Nasal resistance varies widely in neonates and has been reported to contri-bute from 31% to 49% of total lung resis-tance(1). Variations in the cross sectional area, of the nasal cavity have a marked effect on nasal resistance. Newborns are obligate nose breathers and the nasal resistance can modify the magnitude of negative inspiratory pharyngeal pressure which appears to be critical in the develop-ment of obstructive apnea. A decrease in the nasal resistance may reduce the negative inspiratory pharyngeal pressure. The alae nasi (AN) activation appears to be centrally controlled. Phasic inspiratory AN activity is linked with the tonic drive to muscles determining upper airway breathing route(2). Nasal airway receptors have little effect on AN response to hypoxia or hypercapnia but mediate response to nega-tive airway pressure. It is therefore easy to understand that in the absence of any airflow there is unlikely to be generation of negative pressure and hence no activation of AN activity. Choanal obstruction is a potentially remediable cause of respiratory distress. Early recognition with the bedside sign described may be rewarding in most cases. Seema Kapoor,
|
![]()