|
|
Case Reports Indian Pediatrics 2004; 41:496-497 |
||||||
|
Moyamoya Syndrome |
||||||
|
Childhood stroke has varied etiology and it is commonly a result of vascular occlusion(1). Moyamoya disease is a rare type of cerebrovascular disease, which causes stroke in children. Though it is more commonly reported in Japan, it has been sporadically reported all over the world including India(1,2). The characteristic angiographic pattern of ‘puff of smoke’ is diagnostic of Moyamoya disease(3). We describe an association of Moyamoya syndrome with congenital malformations of the eye and eczema. Case Report A 9-year-old girl, the first born of second-degree consanguineous parents, presented with a sudden onset of inability to move the left upper limb and a limp while walking. The onset was preceded by an episode of giddiness and blurring of vision, which lasted for 2-3 hours. The weakness evolved over a period of 12 hours and when she was brought to the hospital, she had dense left hemiplegia and left sided upper motor neuron facial palsy. There was no past history of similar episodes or transient ischemic attacks. There was no history of headaches, vomiting, seizures, loss of consciousness, trauma, ear discharge, recent vaccination, fever or recent diarrheal disease. She had had an itchy, scaling skin rash all over her body since infancy, which had subsided now. She had decreased vision in her right eye from childhood. Her two siblings were normal. Physical examination revealed a conscious, alert child who had inferior coloboma of the right iris and microcornea of right eye (Fig. 1). Both carotid pulses were normal. There was no asymmetry of the limbs. On examination of the central nervous system, higher mental functions were normal. Acuity was reduced in the right eye to perception of movements. Tone was initially decreased on the left side, but later spasticity was present. Clinical course was marked by rapid improvement, and her muscle power improved to 4/5 (MRC grading) by the fourteenth day of hospital stay. Examination of the skin revealed large hypopigmented and hyperpigmented areas all over the body. Active skin lesions were suggestive of atopic eczema. The lesions did not follow any photosensitive pattern of distribution. Nail dystrophy was present, hair was sparse and seborrheic dermatitis of scalp was present.
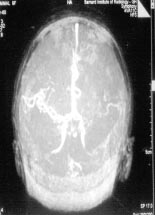
Slit lamp examination of the right eye revealed an inferonasal coloboma of the iris and anterior subcapsular opacities of the lens. Examination of the optic fundus revealed coloboma extending to the optic disc with pigmentation of the borders of the coloboma. Complete blood counts, erythrocyte sedimentation rate, renal and liver function tests were normal. Coagulation profile was normal. Antinuclear antibody was negative. Screening tests for homocystinuria and por-phyria were negative. Serology for leptospira was negative. Chest x-ray was normal and Mantoux test was negative. CT brain showed an infarct in the right parietotemporal region. A right carotid angiogram was performed and the classical ‘puff of smoke’ appearance was seen in the right cerebral circulation (Fig. 2). Magnetic resonance angiogram revealed partially filled up circle of Willis on the left side and occlusion of the circle of Willis on the right side with extensive collaterals (Fig. 3).
Skin biopsy showed features suggestive of atopic eczema with spongiosis of the epidermis and basal cell degeneration mononuclear perivascular infiltrate in the upper dermis. Discussion Moyamoya disease is characterized by stenosis or occlusion of the terminal portions of the intracranial internal carotid arteries and the proximal portions of the anterior and the middle cerebral arteries associated with abnormal vascular networks in their vicinity visible as ‘puff of smoke’ on angiography. Findings of this nature bilaterally is considered definitive for Moyamoya disease; if unilateral is it termed as ‘probable cases(3). Similar findings associated with other septemic conditions is called Moyamoya syndrome. The etiology of this syndrome is unknown and is the source of continuous debate. However, the consensus is that the vascular stenosis is the primary lesion and the consequent cerebral ischemia results in the formation of collaterals(3). The cause for the arterial occlusion is, however, unknown. The associated anomalies and laboratory findings give a clue to the etiology of the disease(3). Association with a particular ethnic group (Japanese), frequency of the disease in siblings and co-existence with other genetic diseases like Down syndrome and sickle cell anemia suggest a hereditary basis for the disease(3). Association of Moyamoya syndrome with malformations of the eye, especially morning glory disc malformations and chorio-retinal colobomas have been reported previously(4-7). This in turn is frequently associated with base of skull malformations like basal meningoencephalocele, panhypopituitarism and midface malformations(6-8). This combination of anomalies of structures in close vicinity like the eye, base of skull and circle of Willis gives a clue that Moyamoya syndrome may be a consequence of a defect at the time of embryogenesis. Skin lesions in the form of livedo reticularis has been reported in association with Moyamoya syndrome (Sneddon syndrome(9)). Association with atopic skin disease has also been reported as a part of cardiofaciocutaneous syndrome(10). The present case showed a coloboma involving the iris and the optic disc, ipsilateral malformation of the cerebral vessels in the form of Moyamoya syndrome and eczema. This combination has not been reported previously. We conclude that it is important to consider the diagnosis of Moyamoya syndrome in a child with stroke and coloboma of the iris. Eczema in association with stroke should also create a suspicion of Moyamoya syndrome and carotid angiography should be performed after thrombocytopenia is excluded. Acknowledgement Prof. J.R. Daniel, Director (Retd.), Barnard Institute of Radiology. Government General Hospital, Chennai 600 003. MRI, MRA and Carotid Angioglram for the child was done under his supervision. Dr. G. Ravichandran, Assistant Professor of Dermatology, Government Stanley Medical College, Chennai 600 001, gave expert dermatological opinion and performed Skin Biopsy for the case. Contributors: MN and MAA managed the patient and drafted the manuscript. RP reviewed the manuscript. Funding: None. Competing interests: None stated. | ||||||
|
References | ||||||
|
|
![]()