|
|
Case Reports Indian Pediatrics 2001; 38: 540-543 |
|||||
|
Oculosporidiosis in Northern India |
|||||
|
Rhinosporidiosis is caused by the Phycomycete Rhinosporidium seeberi and presents as polypoidal and vascular nasal masses(1-2). Ocular involvement occurs in 10% of R. seeberi infections(3). The sites include the lacrimal sac, conjunctiva, sclera, and lids(4). The fungi thrive in hot, tropical climates, and endemic zones are South India and Srilanka(3,5). To the best of our knowledge there is no reported case of oculosporidiosis form Northern India where climatic conditions are different from those prevalent in South India.
An 11-year-old male, a resident of Western Uttar Pradesh, presented with a red and fleshy growing mass in the lower part of his left eye, of 3 months duration. There were associated minor ocular complaints of mild irritation, photophobia and watering from the left eye. No history of any ocular trauma, or contact with animals was present. His past history was unremarkable with no other systemic com-plaints. No obvious cutaneous lesions or lymphadenopathy was present. His un-corrected visual acuity was 6/6 in both the eyes. Right eye examination was within normal limit. The left eye had a solitary mass lesion in its lower medial part, obscuring the left lower lid margin in this area. This lesion was examined by picking up the mass with a gauze piece. The mass was now seen to arise from the inferior bulbar conjunctiva and was red, fleshy and pedunculated with multiple white dots on its surface (Fig. 1). No bleeding or discharge was observed from the surface of the mass. The lesion was freely mobile and firm to touch with no adherence to the under-lying episcleral and subconjuctival tissues. The rest of the ocular and systemic examination was normal. A provisional diagnosis of conjuctival papilloma was made. An excision biopsy of the mass was performed under general anaesthesia by easily snipping the mass off from the peduncle. The biopsy material was sent for histopathological examination. The Hemotoxylin and Eosin stain revealed large chitinous lesions filled with spore like bodies, all embedded in a fibro-myxomatous stroma (Fig. 2). Diffuse infiltra-tion of lymphocytes, monocytes, and plasma cells was seen around these lesions. The connective tissue stroma was covered by stratified squamous epithelium showing mini-mal hyperplasia at places. A diagnosis of Rhinosporidial sporangia in connective tissue matrix was made. The Gram’s stain showed Gram positive, multiple bunched up spores. The conjunctiva adjacent to the area from where the mass had been excised, healed with no evidence of recurrence up to a 6 months follow up period.
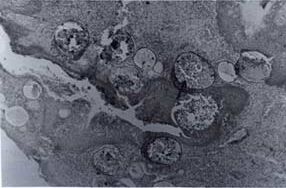
Fig. 2. Histopathological picture of the mass after excision biopsy, stained with H&E stain showing sporangia filled with endospores (arrow) in a fibromyxomatous stroma.
Rhinosporidum seeberi infection is endemic in South India and Srilanka with sporadic reports from various parts of the world including the American continent(3,5). The disease has been found to be associated with animals like horses, mules, cats, dogs and wild ducks(6,7). It is more common in young males probably due to more outdoor activity(1). Conjunctival origin of the disease has been seen in about 7% of the cases with 63% in the age group of 11-20 years(6). The mode of transmission of oculosporidiosis is controversial. It is believed to be dust and air borne and is a disease of the summer months as compared to the nasal infection which is water borne and increasingly encountered in winter months(6). The typical lesion of rhinosporidiosis is fleshy, vascular, polypoidal and granulo-matous(8), greyish white dots, present on the surface of the lesion represent fungal sporangia(5). On histopathology, large chitinous lesions filled with spore like bodies are seen(4). These contain endospores which are released into the host tissue, each maturing in 10 days into a sporangium through an intermediate trophozoite stage(9). The presentation in the eye can be in the form of a swelling in the lacrimal region, a polypoidal conjuctival mass, a lid mass and rarely as a scleral mass which can cause scleral melting(9). Associated systemic involvement has been seen in the form of wart like friable, crenated lesions of the scalp, abdomen, urethra, anus and penis(8). The treatment of oculosporidial conjunc-tival mass is early excision of the lesion along with the surrounding conjuctiva(4). Recur-rences are rare and can be minimized by cauterizing the base of the lesion with 2% silver nitrate solution or alternatively cryopexy can be applied(8). Attempts to culture the causative organism have been un-successful(1,5). In the case reported here, an initial diagnosis of conjuctival papilloma was made because of the papillomatous nature of the mass and also as rhinosporidiosis is not seen in this part of the country. Retrospectively we feel that the white dots on the fleshy lesion were fungal sporangia. Not withstanding geo-graphy, oculosporidiosis should be included in the differential diagnosis of conjuctival polypoidal lesions even in non endemic areas. Ocular infection in such instances may be primary or an individual may be a migrant from an endemic area. Contributors: RA and VR reviewed the literature and drafted the paper. RA will act as the guarantor for the paper. UR and DKM helped in drafting the paper. Funding: None. Competing interests: None stated.
|
![]()