|
|
Original Articles Indian Pediatrics 2001; 38: 461-475 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sero-epidemiology of hepatitis E virus (hev) in urban and rural children of north india |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Manuscript received: March 4, 1999; Initial review completed: October
13, 1999,
Key words: Anti-HEV antibodies, Children, Hepatitis E virus, Seroepidemiology. ENTERICALLY transmitted non A, non B hepatitis has been known to occur in both sporadic and epidemic forms in developing countries(1). The first epidemic was reported retrospectively from New Delhi in 1955(2) and since then many more have been documented from different parts of the world(3,6). Epidemics of hepatitis E virus (HEV) have a high attack rate in young adults in the age group of 15-40 years(7). But studies in children from Sudan(8) and Hong Kong(9) have demonstrated that 12-66% cases of acute sporadic hepatitis seeking care in hospital had IgM anti-HEV antibodies indicating recently acquired infection. From our center(10), 45% patinets with acute liver failure had anti-HEV IgM antibody positivity, of which 27.5% were dual infections of hepatitis A and E. Thus, it is clear that children are sus-ceptible to HEV infection although, exposure and the immune profile may be different from that of adults. HAV and HEV are both spread through orofecal route and thus the exposure probabilities are likely to be similar. Arankalle et al.(11) recently showed that although most of the children acquire anti-HAV IgG antibodies by 5 years of age, the anti-HEV antibody positivity ranged between 0-9% in pediatric population in and around Pune, Western India. On the other hand, HEV seroprevalence in adults was between 16-40%. Because of the smaller number of subjects in their study, it was not possible to assess the susceptibility of children to HEV infection at various ages and determine the changing prevalence of sero-positivity with increasing age. The present study was undertaken to deter-mine the prevalence of HEV infection (anti-HEV IgG antibody status) along with recent (anti-HEV IgM antibody status) infection among children in different age groups and relate anti-HEV antibody status to demo-graphic features which were potential risk factors for acquiring water borne infections.
The study was carried out in the out- patient clinics at the Department of Pediatrics, All India Institute of Medical Sciences, New Delhi (urban) and Comprehensive Rural Health Services Project (CRHSP), Ballabgarh, Haryana (rural) between March to December 1996. It was a cross sectional survey among age stratified pediatric population attend- ing urban and rural health facilities and was essentially a convenient sampling of subjects. HEV is a water borne infection and is widely prevalent in endemic areas. It was therefore assumed that children attending these urban and rural health facilities were representative for the prevalence of HEV infection in their community. In our preliminary seroprevalence study among approximately 200 children in urban and rural areas, IgG antibodies to ORF-3 peptide of HEV were present in 22 to 27% of the subjects. To determine an assumed pre-valence of 25% at an admissible error of ± 2.5%, with 95% confidence, the sample size was estimated to be 1151 children (age range 6 months to 120 months) each for rural and urban strata. In all, 1098 children could be recruited from urban and 1062 from rural areas. Children between 6 months to 10 years of age attending the urban and rural outpatient pediatric clinics for minor non hepatic ailments were recruited. Attempts were made to recruit almost equal number of subjects in each yearly interval for the age. Verbal informed consent was obtained from the parent/accompanying attendant to participate in the study. The study was approved by the institutional ethics committee. A questionnaire was developed in English and Hindi (locally spoken and understood language) which included details about subject identification, age, sex and demographic details (including defecating habits, sewage and waste disposal, water supply and area of residence), reasons for attending the health facilities, duration of breast feeding, parenteral exposure in the past 12 months, history of clinical hepatitis in past and among family members and clinical examination for liver, spleen, presence of jaundice and recording the weight. From each eligible subject, 2 ml blood was withdrawn aseptically into a plain test tube. After clotting, the serum was obtained by centrifugation which was then labeled and stored at –20° C till further processing. Anti HEV IgG and IgM Antibody Assay An in-house developed enzyme immuno-assay system with a synthetic ORF-3 HEV peptide was used to determine anti-HEV IgG and IgM antibodies(12). The method is summarized as below. An immunoreactive ORF-3 HEV peptide (comprising amino acids 91-123) was synthesized using an automated peptide synthesizer (Milligo, Millipore, Bed-ford, MA). After cleaving and deprotection, the peptide was purified by reverse phase high performance liquid chromatography. One microgram of this peptide was coated to each well of a micro-titre plate (NUNC, Kamstroup, Denmark) in 100 µL of carbonate buffer (pH 9.6) at 4° C and incubated at 37° C for 6-12 hours. The un-coated sites were blocked with 5% fat free milk powder (Everyday; Nestle, Mumabi, India) in phosphate-buffered saline (0.05 mmoI/L, pH 7.4) for 1 hour at 45° C. After incubation, the plates were washed three times with wash buffer (Phosphate buffered saline, pH 7.4, 0.05 mmol/L with 250 mmol/L NaCI and 0.1% Tween-20 – BDH, Mumbai, India) The patient sera, diluted 1:20 in phosphate-buffered saline containing Tween-20 (0.1%) and skimmed milk powder (10%) were incubated in peptide coated wells for 1 hour at 45° C. After thorough washing with the wash buffer, 100 microlitre of secondary antibody, affinity purified Anti-Human IgM (µ chain specific)/IgG peroxidase-conjugate (DAKO, the Netherlands) was allowed to react at a dilution of 1:1000 for 45 minutes at 45° C, respectively. The wells were thoroughly washed, and the color was developed using orthophenylene diamine dihydrochloride (Sigma, St. Louis, MO) in citrate phosphate buffer (0.1 mmol/L, pH 5.5) with hydrogen peroxide (0.0006%). The reaction was allowed to continue for 20 minutes and stopped with 50 µL of 2 mmol/L sulfuric acid. The color intensity was read at 490 nm using a Flow-Titretek enzyme-linked immuno-sorbent assay reader (Flow Labs, Scotland). The cut-off value was calculated as half of mean summated positive and negative control. The usual IgM positive samples gave an optical density (OD) value of more than 0.5 and the negative value was below 0.3. Pooled sera samples from epidemics of HEV (Hyderabad) served as positive controls. Sera from 38 infants (6-9 months) was used as negative controls. All these infants were both anti-HEV IgG and IgM negative by commercially available immunoassay kits and RT-PCR test system for HEV RNA. The positive IgG samples gave an OD value of above 1.0 in contrast to the negative value of less than 0.4 OD. A two step validation of the above mentioned in-house developed peptide based HEV ELISA was undertaken(3). 1. In-House validation: Seventy seven individuals with acute viral hepatitis (n = 21) and fulminant liver failure (n = 56) detected to have circulating HEV-RNA (by RT-PCR) were included as positive controls. Two hundred and fifty seven patients who were negative for HEV RNA in RT-PCR assay were taken as negative controls; these were acute hepatitis B (n = 56), acute hepatitis A (n = 27), chronic active hepatitis B (n = 111), chronic hepatitis C (n = 39) and drug induced hepatitis (n = 24). The sensitivity and specificity of the peptide based anti HEV IgM assay so obtained was 88.3% and 98.4%, respectively. 2. Comparison with commercially available kits: The peptide based ELISA was compared with two commonly used commercial kits (Abbot and Genelabs) for detection of anti-HEV IgM. Sera which tested positive and negative with these kits were taken as the positive and negative controls, respectively. Abbot Kit: Out of the 13 positive samples, the in-house ELISA was able to detect anti HEV IgM in 12 (sensitivity 91.3%) and 1 sample was positive out of the 13 negative sera tested (specificity 92.3%). Genelabs kit: Comparison was done in 23 positive and 27 negative controls. The sensitivity and specificity of the peptide based assay was 91.3% and 66.6%, respectively. Definitions 1. Anti-HEV IgG antibodies were estimated in all samples for evidence of HEV infection (both past and recently acquired). 2. Under the assumption that both anti-HEV IgG and IgM antibodies are present in recently acquired HEV infections, anti-HEV IgM antibodies were estimated only in those subjects who demonstrated anti-HEV IgG antibodies as an evidence of new/recent infection. 3. To assess presence of anicteric hepatitis, serum ALT levels were estimated in those subjects who had evidence of recently acquired HEV infection in the form of anti-HEV IgM antibodies. 4. Serum ALT levels were assessed 8-12 weeks after collection of samples. It was stored at –20º C till processing. More than two times the laboratory upper limit for the laboratory (serum ALT ³60 IU/L) was considered as evidence of anicteric hepatitis. 5. Place of residence was described as defined in municipal records, viz., urban, rural and slums. Data Analysis "Stata" statistical package(14) was used to analyze the results. The 95% Confidence Intervals (CI) for proportions, means and medians were also determined. Comparisons were made between various categories using c2 test, Fisher’s exact test, Student ‘t’ test and Mann Whitney U Rank Sum test as appropriate for proportions, parametric or non-parametric continuous data. Differences were considered significant at an alpha of 5% or less. Logistic regression modelling was done for multivariate analysis. Due to missing information, the denomi-nator changed for histories of defecation habits of the child, area of residence, source of drinking water, previous episode of jaundice in the child and immediate family members and parenteral exposure in the past one year. Similarly, in some subjects with anti-HEV IgM positivity, insufficient serum was available for ALT estimation.
I. Baseline Characteristics Out of 2160 subjects recruited for the study, blood samples were available for analysis in 2070 children (95.8%). The baseline features and demographic details of the remaining 90 children whose samples could not be analysed due to insufficiency or hemolysis were similar to the remaining subjects. Thus, during a period of 10 months, data regarding 2070 children (6 months-10 years) attending the urban (n = 1065) and rural (n = 1005) health facilities is presented here. (Table I). The study subjects were uniformly distributed in the various age categories. The two populations were significantly different with respect to several demographic features. Past history of jaundice, both in the index child and immediate family members was more often elicited in those children attending the urban facility as compared to those recruited from the rural dispensary (p = 0.042 to 0.001). Study subjects at the urban facility also had more frequent history of parenteral exposure than the rural children (p = 0.000). Table I__Baseline Characteristics of Study Subjects from Urban and Rural Health Facilities
* median: (95% binomial exact Confidence Interval)
[applied Wilcoxan Rank Sum Test (WRS)]. II. HEV Seroprevalence Studies IIA. Urban Data IIA1. HEV Infection Status (Table II) (i) Anti-HEV IgG antibody status (Table II) IgG antibodies to HEV were present in all age categories and showed an increasing prevalence rate from one year (14.2%; 95% CI, 7.6-20.7) till 10 years (38%; 95% CI 31.7 = 44.3) of age. The prevalence was signi-ficantly higher among those who were more than 48 months (228/650; 35.1%; 95% CI 31.4-38.8) than those less than 48 months (78/415; 18.8%; 95% CI 15-22.6) (p = 0.00). (ii) Anti-HEV IgM antibody status (Table II) Anti-HEV IgM antibodies were estimated in those subjects who had anti-HEV IgG antibodies. In these subjects, anti-HEV IgM positivity ranged between 14.3-50.7% in different age groups (p = 0.165). Recently, acquired infection was observed in 35.9% children (28/78; 95% CI 25-46.8) below 48 months of age and 45.2% (103/228; 95% CI 38.7-51.7) in those older than 48 months (p >0.15). As a proportion of total subjects, evidence of recently acquired infection was 4.4% (5/113), 2.1% (2/96), 10.1% (21/206), 14.6% (31/213), 17.8% (37/208) and 15.3% (35/229) in 6-12, 13-24, 25-48, 49-72, 73-96 and 97-120 months age categories, respectively. Overall, 12.3% (131 out of 1065) children from urban area had anti-HEV IgM antibodies. Table II__Anti-HEV IgG Antibody Status in Relation to Age in Urban and Rural Children in North India
* IgM antibody were estimated in those children who were anti-HEV IgG
antibody positive (iii) Serum Alanine Aminotransferases (ALT) Median serum ALT levels were 11 IU/L (95% CI 11-11) in 120 children with anti HEV IgM antibodies in whom sera was available. In 9 children (7.5%; 95% CI 2.7-12.3) these were more than twice the upper normal limit for the laboratory (>60 IU/L). None of these children had clinical evidence of jaundice.
Anti-HEV IgG antibody positivity was not related to the sex, nutritional status, duration of breast feeding, number of household mem-bers, parental education, place of residence, sewage disposal for the child and family and source of drinking water (p = 0.19 to 0.897). Past history of jaundice was present in 4.9% (15 out of 303) of anti-HEV IgG positive group as compared to 5.1% (38 out of 740) in antibody negative group (p = 0.907). There was no significant difference in the history of jaundice in immediate family members of the two groups (anti-HEV IgG positive group 27/302, 9% vs antibody negative group 54/735, 7.3%) (p = 0.47). History of parenteral ex-posure in the form of injections, IV fluids or transfusion of blood products was similar in antibody positive (33/220, 15%) and antibody negative (72/376, 19.1%) categories (p = 0.199). IIB. Rural Data IIB1. HEV-Infection Status (Table II) (i) Anti-HEV IgG antibody status: Similar to the urban study subjects, IgG antibodies to HEV were present in all age categories and showed an increasing prevalence rate from infancy (7.2%; 95% CI 2-12.4) to 10 years (33.3%; 95% CI 26.7-40) (p = 0.000). The prevalence of HEV IgG antibodies was significantly higher among those who were more than 48 months old (179/602;29.1%; 95% CI 26.1-33.4) than those younger than 48 months of age (60/403; 14.9%; 95% CI 11.4-18.4) (p = 0.0000). (ii) Anti-HEV IgM antibody status (Table II): Among children with anti-HEV IgG antibody, prevalence of anti-HEV IgM antibodies varied between 0% to 64.3% in different age groups. The exposure probability to recently acquiring infection almost doubled from 25% (15/60; 95% CI 13.7-36.2) before the age of 48 months to 54.7% (98/179; 95% CI 47.4-62.1) after the age of 48 months (p = 0.0000). As a proportion of total subjects, evidence of recently acquired infection was 0% (0/97), 1.8% (2/107), 6.5%(13/199), 13.1%(28/213), 18.5% (36/194) and 17.4% (34/195) in 6-12, 13-24, 25-48, 49-72, 73-96 and 97-120 months age categories, respectively. Overall, 11.2% (113 out of 1005) children from rural area had anti-HEV IgM antibodies. (iii) Serum alanine aminotransferases (ALT): Median serum ALT levels were 9 IU/L (95% CI 7-9) in 88 children with anti HEV IgM antibodies in whom sera was available. In 5 children (5.5%; 95% CI 1.9-12.8) these were more than twice the upper normal limit for the laboratory (>60 IU/L). None of these children had clinical evidence of jaundice.
Rural children with anti-HEV IgG antibodies were more frequently defecating in open/community latrines (135/239, 56.5%) as compared to those who were anti-HEV IgG antibodies negative (347/763, 45.4%) (p = 0.003). Past history of jaundice was present in 5% (12 out of 238) of anti-HEV IgG positive group as compared to 2.6% (20 out of 763) in antibody negative group (p = 0.06). There was no significant difference in the history of jaundice in immediate family members of the two groups.
In urban center, the study subjects had sought care for fever (23.7%); diarrhea (13.5%); acute respiratory infection (8.5%); pyoderma (0.7%); vaccinations (11.3%); malnutrition (17.3%) and other miscellaneous complaints (25%). At rural center, the reasons for coming to health center were fever (26.8%); diarrhea (10.5%); acute respiratory infection (10.5%); pyoderma (24.3%); vaccination (0%) and other miscellaneous complaints (27.9%). Conditions for which subjects were attending the outpatient clinics at the rural and urban health facilities were distributed similarly in anti-HEV antibody positive and negative groups (p = 0.169 to 0.855).
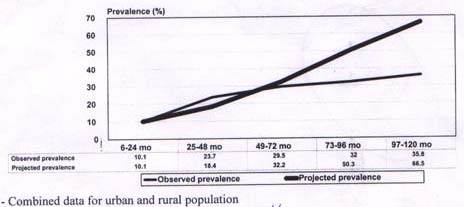
The study subjects were recruited between the months of March to December 1996. Anti-HEV IgG and IgM antibody positivity were found in all the study months except December and there was no unusual upsurge of either IgG or IgM anti-HEV antibodies in any particular month of season (p = 0.42). Multivariate Analysis In a logistic regression model, age categories ( £ 48 months and >48 months), sex, maternal education, sewage disposal, defecating habits and illness at presentation (diarrhea yes/no) were entered as explanatory variables and anti-HEV IgG antibody positivity as outcome variable. For predicting anti-HEV IgM antibody positivity, in addition to the above variables, family history of jaundice was also entered as an explanatory variable. The odds ratio of HEV IgG positivity was 2.33 (95% CI 1.7-3.13; z = 5.65, p = 0.000) in urban children and 2.42 (95% CI 1.75-3.35; z = 5.32, p = 0.000) in rural subjects if age was more than 48 months. No other explanatory variable significantly predicted presence of anti-HEV IgG antibody. Anti-HEV IgM was significantly associated with older age category (>48 months) only in rural children (odds ratio 3.1; 95% CI 1.6-6.1; z =3.24, p = 0.001). No other explanatory factors were associated with presence of HEV antibodies. Weaning off of Anti-HEV IgG Antibodies It was a cross-sectional study and hence the duration of persistence of anti-HEV IgG antibodies could not be ascertained with confidence. However, it was assumed that the study subjects were part of a steady population where no epidemic of HEV was going on and, that anti-HEV IgG antibodies would persist throughout childhood once these appear. Under these assumptions, some projections about the expected prevalence could be made and compared with the observed prevalence (Fig. 1). The expected antibody prevalence (combined for rural and urban areas) was computed in the following manner: (a) IgG antibody prevalence in 6-24 months was taken as the basal value and thereafter, (b) prevalence of IgM antibody in subsequent 2 year age intervals till 10 years were sequentially added. For example, anti-HEV IgG was present in 42/413 (10.1%) children in 6-24 months age category. Anti-HEV IgM antibody was present in 34/405 (8.3%) in 25-48 month age group category which represented recently acquired HEV infection. Proportion who acquired the infection recently and those who were infected with HEV in previous age group should together constitute the total HEV antibody positivity in this group. Thus, for 25-48 months expected total anti-HEV IgG positivity would be (8.3% + 10.1% = 18.4%) provided IgG antibodies were to persist perpetually after appearing once. Thereafter, for every subsequent age interval, prevalence of IgM antibody was added up so that in 97-120 months age group the expected anti-HEV antibody prevalence was 66.5% compared to the observed of 38%. The difference between expected and observed antibody prevalence would represent the proportion of subjects in that age category in whom antibody weaned off. As can be seen in Fig. 1, that after 4-6 years of age, the deficit between expected and observed prevalence increased from 2.7% to 31% by 10 years.
In the present study, children from urban (n = 1065) and rural (n = 1005) health facilities between the age of 6 months and 10 years were screened for anti-HEV IgG and IgM antibodies. The study demonstrated that exposure to HEV started occurring in the first year of life and that anti-HEV IgG antibody positivity progressively increased till 10 years in both urban and rural children (Table II). Overall the seroprevalence of IgG antibodies against HEV were significantly more in urban as compared to that in rural subjects (p = 0.011).
Fig. 1. Weaning off of anti-HEV IgG antibodies - projected versus observed prevalence* The probability of carrying anti-HEV IgG antibody increased by over two folds in those above 48 months of age as compared to younger children [rural OR-2.45 (95% CI 1.75-3.35) and urban OR-2.33 (95% CI 1.7-3.13)]. This indicated increased probability of exposure to HEV during school age group. It was particularly true in rural areas where prevalence of IgM antibodies was significantly higher in >48 months age group (OR 3.1; 95% CI 1.6-6.1) as compared to those in younger age group (p = 0.001). The possibility of some children below 12 months having anti-HEV IgG antibodies of maternal origin cannot be ruled out. This may be the reason that anti-HEV IgG prevalence remained either static (urban) or declined (rural) between 6 months to 24 months age group. However, in urban areas there were infants with anti-HEV IgM antibodies indicating postnatally acquired infection. In contrast there were no infants <12 months with anti-HEV IgM antibodies in rural areas. This may be due to longer duration of breast feeding in rural areas which in turn would reduce the risk of all water borne infections(15). During the study period. no hepatitis epidemics occurred in the area, but sporadic cases of acute hepatitis continued to attend the pediatric outpatient of urban hospital as well as the rural dispensary. Anti-HEV IgG antibodies were identified uniformly without any seasonal or monthly peaks in samples obtained throughout the year. In all, 244 out of 545 children with IgG antibodies (44.8%; 95% CI: 40.5-49.0) had evidence of recent infection (i.e.,anti-HEV IgM antibodies). This constituted 11.8% (244 out of 2070; 95% CI 10.4-13.2) of the total study population. In a recent study by Wei et al., individuals with acute HEV infection had IgM antibodies without concurrent IgG antibodies(16). Since IgM anti-HEV anti-bodies were not estimated in all subjects, the prevalence of recently acquired infection in pediatric population in the present study may actually be an underestimate. Native HEV infection has been described from almost all parts of the world, including industrialized nations(17-20). Seroprevalence of HEV infection is low and varied between 1-7% in countries like Australia(17), Germany(18), France(20) and The Nether–lands(21). In contrast, the seroprevalence rates in Asia(11,22-24), Africa(25-27) and South America(28,29) are higher and ranged between 5.5% to 71% in various studies. The seroprevalence in children in our study was similar to that observed in other Asian countries. The socio-economic status and sanitary conditions prevailing in the commu-nity may explain the major differences in the prevalence patterns seen across the regions. There are only a few studies estimating serological evidence of exposure to HEV in non-icteric children. Report from Pune, Western India(11), Kathmandu, Nepal(30), Egypt(31,32), Chile(29), Sudan(8) and Lucknow, North India(33) showed a wide range (0-64%) of seroprevalence rates to HEV infection. These studies are from regions endemic for HEV and where epidemics have also been described. In Pune, Western India(11), the prevalence of anti-HEV IgG antibodies was 0-9% in the first decade of life; none of the 20 children below 18 months had these antibodies. Similarly, neither IgG nor IgM antibodies were detected in 99 children in Kathmandu, Nepal(30). In contrast to the low sero-prevalence reported from two regions of the Indian Sub-continent, 28.7% urban and 23.8% rural children below 10 years in North India in the present study had anti-HEV IgG antibodies. Aggarwal et al. from Lucknow, North India, detected HEV antibodies in 64% (95% CI 30.6-69.3) of children below 5 years and in 59% (95% CI; 36.3-79.2) between 6-10 year of age(33). In the two studies from Egypt(31,32) and a study from Sudan(8), the prevalence of anti-HEV antibodies was between 0-25% in asymptomatic control children. This wide variation in seroprevalence may be explained by differences in the distribution of virus between regions and within the region. In addition, risk factors which determine the exposure of the child to HEV may also vary with the study sites. Although, hepatitis E epidemics have been described from all parts of the Indian Sub-continent, some of the largest epidemics have been described from North India(6,34). This might be due to widespread distribution of virus in this region. Hence, as demonstrated in our study, exposure to HEV started occurring right from infancy and a significant proportion in urban and rural areas were seropositive in childhood. This was consistent with the findings of Aggarwal et al.(33). Another possibility for observed differ-ences in the seroprevalence rates of HEV-antibodies within the Indian Subcontinent may be the use of antigens from diverse strains and components of HEV in the enzyme immuno-assay systems in different studies(11,30, 35,37). We used a synthetic peptide compris-ing amino-acids 91-123 of HEVORF-3. The sequence of the peptide was based on the HEV strain isolated from Hyderabad epidemic(38). Although, in the study by Mast et al.(39), synthetic peptide (ORF 3) assays were considered less sensitive, in our own studies the test had both high sensitivity and specificity. Precision of estimates of seroprevalence would also depend on the number of subjects studied in the published reports so far. The number of subjects in pediatric age group in published studies so far were too few in each age category as compared to this study wherein approximately 100 children were screened for every one year age interval till 10 years. HAV and HEV are both feco-orally transmitted infections which cause similar acute self limiting illnesses and no chronic sequelae. In the present study, the sero-positivity to anti-HEV IgG increased progressively from 7.2-14.2% in infancy to 33.3-38% by 10 years of age in rural and urban children, respectively. This pattern of increasing seropositivity was very similar to HAV epidemiology published from the region(11,40), albeit lower proportion of children seroconverted. This may be explained by failure of young children to mount a brisk anti-HEV response or a larger dose of virus may be required to cause infection or else rapid decay of anti-HEV antibody occurring after initial acquisition of infection. There is uncertainty over how long HEV antibodies persist. Therefore evaluation of seroprevalence based on the presence of antibodies is difficult to interpret. Reports have suggested that HEV antibodies are short lived, lasting for 0.5 to 4.0 years(11,41,42). Khuroo et al. reported persistence of HEV antibodies for 14 years after an epidemic(43), however re-exposure to HEV in the intervening period in an endemic environment cannot be excluded. Our data does suggest that anti-HEV antibodies declined over time (Fig. 1). Anti-HEV IgM antibodies are reported to last for 3-6 months after an acute infection (30, Kamili S., et al. unpublished data). Thus, if IgG antibodies were long lasting, their prevalence would have increased proportionately to the fresh infection acquired in the previous age categories (Fig. 1). But this was not observed. Since the present study was not a longitudinal cohort study, the projections about expected prevalence of anti-HEV IgG antibodies and the difference between projected and observed prevalence would be of hypothesis generating value. If we assume that the study subjects came from a steady population, then it appeared that probability of weaning off of anti-HEV antibodies gradually increased throughout childhood and almost a third of children were losing IgG antibodies by 10 years of age (Fig. 1). In the hypothetical model, we noticed that the expected and observed lines separated widely after the age of 4-6 years and hence this would be the estimated duration of persistence of antibodies. Weaning off of HEV antibodies is likely to make individuals susceptible to re-infection and development of clinical illness particularly during epidemic situations. Among those with anti-HEV IgM anti-bodies, 7.5% (95% CI 2.7-12.3) urban and 5.7% (95% CI; 1.9-12.8) rural children had increased ALT levels indicating anicteric hepatitis. ALT levels decline over time when sera is stored even at –20°C(44). Hence, these results are likely to be a conservative estimate of anicteric hepatitis following HEV infection. We are not aware if anyone of these subjects developed icterus subsequently since, there was no organized follow up of these patients. Overall, past history of jaundice was present in about 5% of anti-HEV IgG positive children in both urban and rural areas. Similar proportion of children without anti-HEV antibodies also had history of jaundice in the past. Etiological spectrum of acute sporadic viral hepatitis in children attending the same urban hospital and rural dispensary during the period when seroepidemiology samples were obtained demonstrated that 48% of the episodes were due to acute HAV and 13% episodes due to acute HEV infection. The data hence indicated that HEV infection in childhood is mild and mostly subclinical forms are prevalent. The findings are consistent with earlier reports(11,45,46). The study design incorporated demo-graphic features that could be potential risk factors to acquire anti-HEV IgG antibodies. However, none of these were related to anti-HEV status of the child. This may be either due to wide distribution of virus in a heavily contaminated environment and prevailing poor hygenic conditions or related to other un-identified risk factors. In rural area, defecation by the child outisde the house appeared to be having a weak association (OR-1.7 95% CI 0.96-2.9; p = 0.068) with a recent HEV infection (IgM-antibodies). The major limitation of the study was its sampling procedure. Children attending the outpatient department of a tertiary care urban hospital and a rural dispensary for minor illnesses were the subjects for the present study. This was likely to restrict the general application of the study. In multivariate analysis, none of the factors for which children came to health facility were significantly associated with anti-HEV antibody status. The rural center provided health services to a population of 1,25,000 people in rural Haryana. Similarly, only children residing in South Delhi colonies were recruited from urban hospital. The objective was to have study sample from a predefined population. In conclusion, children were exposed to HEV early in life and, serpositivity progressively increased upto the age of 10 years in North Indian urban and rural children. There were no rural and urban differences in exposure probabilities to HEV during childhood. One-fourth to one-half of the HEV-infection was acquired recently as indicated by the presence of anti-HEV IgM antibodies. However, anti-HEV IgG antibodies appeared to be short lasting. Most of the HEV infection in childhood was mild and remained sub-clinical. Acquiring anti-HEV IgG antibodies or anti-HEV IgM antibodies was not related to demographic features identified as potential risk factors. Continuous efforts to improve sanitation, and personal hygiene along with provision of clean drinking water to the communities in developing countries are necessary interventions to control exposure to HEV and other water borne infections.
We acknowledge the support of Dr. Seema Joshi and Dr. Medha Deo in collecting samples. Contributors: NKA designed and co-ordinated the study, analyzed the data and drafted the manuscript. He will act as the guarantor for the study. SKK and MI were involved in data collecton and sample processing. SKP, BLJ and MI provided laboratory support. PM collected data, processed the samples, analyzed the data and helped in preparing the manuscript. Funding: Indian Council of Medical Research. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()