|
Case Reports Indian Pediatrics 2000;37: 549-552 |
|||||||||
|
Candidial
Intestinal Perforation in a Non-Immunocompromised Infant
|
|||||||||
|
Suravi
Mohanty
Usha Kini From the Department of Pathology, St. John’s Medical College, Bangalore 560 034, India.
Intestinal perforations are most often non-specific occuring as a sequalae of ischemia and gangrene or could be associated with enteric fever. However, perforations caused by specific etiologic agents such as fungi are extremely rare. They have occasionally been diagnosed in immunocompromised individuals or low birth weight neonates. We report a 11 month old non-immunocompromised male child with intestinal candidiasis complicated by perforation.
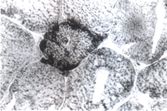
An 11-month-old male child was admitted to St. John’s Medical College Hospital with the history of irregular, low grade fever, severe abdominal pain and diarrhea of 10 days duration prior to which he was treated symptomatically by a local doctor for 4 days with no improvement. There was no associated vomiting. On examination, the child was moderately built and nourished. He was febrile and mildly dehydrated. Abdominal distension was observed with minimal free fluid. The blood cell counts were within normal limits. An aspirate of the peritoneal fluid showed straw colored transudate with a total cell count of 100 cells/cu mm comprising lymphocytes. The patient was treated symptomatically but at the end of 5 days, the abdominal pain worsened. The abdominal distension progressed further. On examination, the liver dullness was obliterated with the abdominal X-ray showing gas under the diaphragm. The bowel sounds were absent and the patient became toxic. A repeat peripheral blood examination at this time showed leukocytosis with relative lympho-penia. With a clinical diagnosis of intestinal per-foration, the patient was taken up for an emergency laparatomy. A single perforation site measuring 1 ´ 0.5 cm was identified in the ileum. The rest of the intestine and other abdominal viscera appeared grossly normal. Swabs were taken from the perforation site and peritoneal wall for routine culture studies. The perforation site with the viable margins was resected. Eight centimeter long resected segment of ileum with the site of perforation was sent for histopathologic examination. The perforate measured 1 cm in greatest dimension and the edges were covered by exudate. The rest of the intestine was grossly normal. At microscopy, the edges of the perforation which were covered by fibrinous exudate showed numerous branching pseudohyphae with invasion into the adjacent viable granulation tissue. A few sporulating forms morphologically similar to blastospores of candida were also seen (Fig. 1). These fungal structures were ratified with Gomori’s silver methenamine and periodic acid-Schiff stains. Multiple sections taken from the rest of the intestinal wall were unremarkable. Microbiological studies on the swab material confirmed the growth of Candida albicans. A histopathological diagnosis of candidial intestinal perforation was made. As the fungal hyphae showed tissue invasion, the patient was treated with keto-conazole and intravenous metrogyl infusion. He made a steady progress and was fit and well at the time of discharge from the hospital.
Gastrointestinal candidiasis in humans is the commonest fungal infection which could involve practically any site of the alimentary tract. It normally presents as superficial ulcers involving only the mucosa, most commonly affecting the gastro-esophageal junction. But intestinal involvement is very unusual and is most often encountered only at post mortem examination in immuno-compromised individuals. Over a period of 33 years from 1966 to March 1999, 1,29,367 general surgical biopsies were received at the general pathology Department of the Institution. Of these, 84 were all non-specific intestinal perforations diagnosed only in the neonates and infants accounting for a frequency of 0.065% among the neonates. To the best of our knowledge, this is the first case of its kind in English literature to report on candidial intestinal perforation in a non-immunocompromised infant. The patient in the present context was a perfectly normal child, moderately built and nourished and had no evidence of immune suppression. Tests for tuberculosis and HIV infection were negative. The serum protein levels were within normal limits. The parents’ blood samples for HIV infection were also negative. Earlier reports of candidial intestinal perforations have been described only in extremely low birth weight infants(1,2) and in patients who have undergone ventriculo-peritoneal shunts(3). In these cases, the perforations seen at laparatomy were focal, often multiple and situated on the antimesentric border of the distal ileum. None of the infants showed any features of necrotising enterocolitis. Novack et al.(2) have found positive cultures for either Candida albicans or Staphylococcus epidermidis in only four of the 11 infants with intestinal perforation and none in those infants without perforation. In a study of 2517 autopsies, 109 revealed histologically documented candidial involvement in the gastrointestinal tract(4). In the pathogenesis of candidiasis, colonisation was considered as the essential first step. Antibiotics, corticosteroids, H2 blockers, antacids, T cell dysfunctional states, burns, diabetes mellitus, irradiation and chronic renal disease are most frequently cited as risk factors for colonisation. Once colonisation has been established candida organisms result in localized infection resulting from disruption of integrity of the gastrointestinal mucosa assisted by factors such as cytotoxic chemotherapy, graft versus host disease as well as hypotension(5). We conclude that focal gastrointestinal perforations occuring in an infant with normal immune status does represent a clinically distinct phenomenon and that these perforations may be associated with candida and/or Staphylococcus epidermidis infections. The finding at operation of isolated focal intestinal perforation without intestinal distension and bowel wall thinning or discoloration is quite characteristic of gastrointestinal perforations due to candida in non-immunocompromised individuals.
|
|||||||||
![]()