|
Case Reports Indian Pediatrics 2000;37: 540-542 |
|||||||
|
ANA
Negative Lupus Erythematosus
|
|||||||
|
K.K. Locham Jaswir Singh Rajinder Garg Manjit Singh Chanchal Jain*
Systemic lupus erythematosus (SLE) is an inflammatory disease with multisystem involvement and a varied clinical presentation. The presence of antinuclear antibodies (ANA) in serum is generally considered a decisive diagnostic test for SLE. ANA negative SLE seems to be a subgroup of SLE that is infrequently recognized. We report one such case.
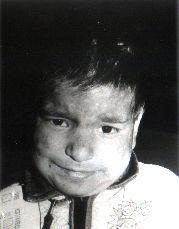
A 6-year-old girl presented with recurrent multiple cutaneous lesions mainly present on scalp, face, palms and soles (but sparing other parts of the body) of 10 months duration. Scalp showed diffuse erythema, scaling and at places crusting. Face showed discrete, erythematous, maculopapular, telangiectatic eruptions on the forehead, ears, butterfly area of the cheeks. Both eyelids showed scaling and crusting. Both lips were edematous with blurring of the vermilion border and were covered with thick hemorrhagic crusts. Lesions on palms and soles were sharply demarcated in the form of reticulate telangiectactic erythema on thenar and hypothenar eminences (Fig. 1). There was history of photosensitivity and pain in knee joints not accompanied by any swelling or redness. There was accompanying fever. The patient also complained of pain in epigastrium and malena for last 3 months. Apart from hepatosplenomegaly, the systemic examination was unremarkable. Investigations revealed a hemoglobin of 5 g/dl and peripheral blood film showed microcytic hypcohromic red blood cells with marked anisocytosis and poikilocytosis. Total leukocyte count was 9400 cells/cu mm with 71% polymorphs, 27% lymphocytes and 2% monocytes and ESR of 60 mm in the first hour. Platelet count at the time of admission was 1,20,000/mm3 which decreased to 40,000/mm3 after 1 week and 3 weeks, respectively. Bleeding and clotting times were normal. Urine examination showed protein in traces. Total serum proteins were 5 g/dl; albumin 3 g/dl and globulin 2 g/dl. Serum glutamic oxaloacetic transaminase was 138 IU/L and serum glutamic pyruvic transaminase was 41 IU/L. Renal functions were within normal limits. Anti-streptolysin titer was negative. Test for antinuclear antibodies done by ELISA was negative. Lupus erythematosus cell phenome-non was absent. Venereal disease research laboratory (VDRL) test was weakly positive. Biopsy from one of skin lesions was not contributory. Blood culture revealed growth of Staphylococcus aureus and pus culture from skin lesion grew Klebsiella pneumoniae. Due to non availability of tests, serum antibodies to ds-DNA, serum levels of C3, C2 and C4 and immunofluoroscent test on skin biopsy could not be done. The patient was put on treatment with ampicillin and gentamicin for 10 days and prednisolone was continued for 2 weeks. After treatment the lesions healed with hypo-pigmented depressed scars but telangiectasia still persisted at places. Ten days after withdrawl of steroids similar lesions appeared on face, hands and feet (Fig. 2). The patient was put on injection methyl prednisolone for 3 days followed by maintenance therapy of pred-nisolone. There was improvement in skin rash.
Systemic lupus erythematosus character-istically affects many organ systems and is associated with a variety of immune pheno-mena. Diagnosis of SLE is usually made if any four or more of the eleven criteria are present(1). In the present case five criteria were present in the form of malar rash, discoid rash, photosensitivity, oral ulcers and thrombo-cytopenia. Cutaneous involvement is usually the predominant feature of antinuclear antibody negative SLE(2). In our case also cuteneous involvement was marked and antinuclear antibodies were negative. Cutaneous lesions were localized to scalp, face, palms and soles. In a series of 40 cases reported from Lahore, skin lesions were noted in 85% of cases but palmar erythema was rare and antinuclear antibodies were positive in 80% of cases(3). However, in the present case palmar erythema was marked and antinuclear antibodies were negative. In another series of ANA negative patients with SLE cutaneous symptoms were infrequent while thrombocytopenia and positive VDRL test were a frequent finding(4). In the present case thrombocytopenia was present and VDRL test was weakly positive. Other features reported in ANA negative SLE are hair fall, Raynaud’s phenomenon, recurrent oral ulcers, lupus nephritis, oculo-motor palsy and penile ulcer(5-7). ANA negative SLE patients may show antibodies to double stranded DNA (anti ds DNA)(8). Similarly, in few cases of lupus, negative serological tests do not always exclude SLE as these tests may become positive at a later period(9).
|
![]()