S.B. Bavdekar
P. Vaideeswar*
R.H. Bukane
D.K. Sahu
J.R. Kamat
From the Departments of Pediatrics and
Pathology*, Seth GS Medical College and K.E.M. Hospital, Parel,
Mumbai 400 012, India.
Reprint requests: Dr. S.B. Bavdekar, A2-9,
Worli Seaside CHS, KAG Khan Road, Worli, Mumbai 400 018, India.
Manuscript Received: April 8, 1999;
Initial review completed: May 3, 1999;
Revision Accepted: August 22, 1999
Aneurysms of the aorta rarely occur in
children, usually in association with inherited connective tissue
disorders(1). Aortic aneu-rysms have also been reported in
tuberous sclerosis, but infrequently. We report an association of
tuberous sclerosis with a large thoraco-abdominal aortic aneurysm
with a brief review of literature.
Case Report
A 6-year-old boy previously diagnosed to have
tuberous sclerosis in infancy on the basis of mental retardation,
Shagren patch, myoclonic epilepsy, and CT scan of the brain, was
admitted for progressive dyspnea. The patient’s vital parameters
were unstable and examination showed manifestations of tuberous
sclerosis such as Shagren patch and adenoma sebaceum. He had a
firm pulsatile mass in the epigastric region extending upto the
umbilicus. Chest radiography, ultrasonography, and aortogram (Fig.
1) revealed a large multilobed aneurysm of the descending
aorta distal to the origin of the left subclavian aretery, and
extending upto the infra-renal portion. The distal abdominal aorta
was unaffected. The patient’s condition deteriorated and he
expired before therapeutic surgical intervention.
At autopsy, a fusiform, multilobed aneu-rysm
was seen to involve 15 cm long segment of the thoracoabdominal
aorta (Fig. 2). There were two saccular protrusions. The
proximal sac (8´7´5
cm) was adherent to the left lung while the distal sac (7´6´5 cm)
contained the mildly stenotic ostia of the celiac, superior
mesenteric and renal arteries. The aneurysm had a thick and
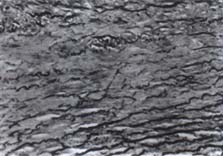
fibrotic wall with lumenal thrombi. Micro-scopically, sections of
the non-aneurysmal aorta revealed increased collagen and ground
substance in the media with a paucity of elastic fibers (Fig. 3).
The vasa vasora in the adventitia showed no changes. Visceral
arteries had normal histology. Other autopsy findings included
cortical and periventricular tubers in the brain, cysts and
angiomyolipomas in the kidneys and fascial angiofibroma around the
left eleventh intercostal muscle. Heart did not reveal any
rhabdomyoma.
|

|

|
|
Fig. 1. Aortographic film showing thoracoabdominal
aneurysm. |
Fig. 2. Large aneurysm (A) involving thoracic (T) and
abdominal aorta and dwarfing the heart (S–left subclavian
artery, L–apex of the left lung). |
|
|
|
Fig. 3. Non-aneurysmal thoracic aorta, media with increased
collagen and patchy paucity of elastic laminae (Elastic van
Gieson, X250).
|
Discussion
Tuberous sclerosis has protean manifesta-tions
and is characterized by hamartomas in many organs, especially the
brain, kidneys, eyes, and bones. Aortic aneurysm, as an additional
feature in setting of tuberous sclero-sis, has been rarely
reported. The first two cases were reported in the French
literature(2) and subsequently a handful of cases have appeared in
the English literature(3-11). The majority have occurred in
children below the age of five years and involving the abdominal
aorta with an exception each where it occurred in a 24-year-old
man(8) and in the thoracic aorta(9). Ours is probably the first
case wherein both thoracic and abdominal portions of the aorta
have been involved.
Several hypotheses have been put forth
regarding the genesis of these aneurysms. Vascular dysplasia of
medium sized arteries may represent a manifestation of tuberous
sclerosis(5). Similarly, dysplasia can also involve the vasa
vasora leading to weakening of the aortic wall and aneurysm
formation(5). Some have likened histological changes with those
seen in Marfan’s syndrome(10). It has also been reported that
hemodynamic stresses produced by hypertension coupled by bilateral
medial fibromuscular dysplasia of common iliac arteries produce an
aneurysm in the infra-renal portion of abdominal aorta(4). The
aorta in the reported case showed alteration in the medial
architecture suggesting presence of connective tissue disorder.
Considering the reported cases and the fact
that aneurysm of the aorta in a child with tuberous sclerosis has
been successfully tackled surgically(10,11), it would be
worthwhile screening these patients for early detection of
aneurysm of aorta. This would prevent unto-ward outcomes,
especially rupture(9). For detection, given their availability,
non-invasive nature, and sensitivity, chest radiography and
ultrasonography could be the preferred screening tools.
Acknowledgements
Authors thank Dr. P.M. Pai, Dean, Seth GS
Medical College and K.E.M. Hospital for permission to publish the
report. They also express their gratitude to Dr. A.P. Desai and
Dr. Jayshree Sharma of the Department of Pathology of these
institutions for the valuable help rendered.
1. Defraigne JO, Paquot JP, Creemens E, Limet
R. Aneurysm of the abdominal aorta in an eighteen-month old
child. Ann Vasc Surg 1988; 2: 193-195.
2. Freycon F, Mollard P, Hermier M. Aneurysme
de I’aorte abdominale au cours d’une sclerose tubereuse de
Bourneville Pediatrie 1971; 26: 421-427.
3. Dutton RV, Singleton EB. Tuberous
sclerosis: A case report with aortic aneurysm and unusual rib
changes. Pediatr Radiol 1975; 3: 184-186.
4. Hagood CO, Garvin DD, Lachina FM.
Abdominal aortic aneurysm and renal hematoma in an infant with
tuberous sclerosis. Surgery 1976; 79: 713-715.
5. Rolfes DB, Towbin R, Bove KE. Vascular
dysplasia in a child with tuberous sclerosis. Pediatr Pathol
1985; 3: 359-373.
6. Towbin RB, Ball WS, Kaufman RA. Abdominal
aortic aneurysm in a patient with tuberous sclerosis.
Radiographics 1987; 7: 818-821.
7. Chao TY, Lee CH, Chiang YC, Tsai YH, Lan
RS, Shieh WB, et al. Tuberous sclerosis with unusual rib
deformity and abdominal aortic aneurysm. Chang-Keng-I-Hsueh
1988; 11: 145-151.
8. Ng SH, Ng KK, Pai SC, Tsai CC. Tuberous
sclerosis with aortic aneurysm and rib changes. J Comput Assist
Tomogr 1988; 12: 666-668.
9. Shephered CW, Gomez WR, Lie JT, Crowson
CS. Causes of death in patients with tuberous sclerosis. Mayo
Clin Proc 1991; 66: 792-796.
10. Van Reedt Dortland RW, Bax NM, Huber J.
Aortic aneurysm in a 5-year-old boy with tuberous sclerosis. J
Pediatr Surg 1991; 26: 1420-1422.
11. Tsukai A, Noguchi R, Honda T, Tabita T, Fukada S, Shimoji
K. Aortic aneurysm in a 4-year-old child with tuberous
sclerosis. Pediatr Anaesth 1995; 5: 67-70.
|
