Munni Ray
Pratibha Singhi
Prabhjyot Malhi
Anil Bhalla
From the Division of Pediatric Neurology,
Department of Pediatrics, Advanced Peditric Center, Post
Graduate Institute of Medical Education and Research, Chandigarh
160 012, India.
Reprint requests: Dr. Pratibha D. Singhi,
Additional Professor, Department of Pediatrics, Post Graduate
Institute of Medical Education and Research, Chandigarh 160 012,
India.
Manuscript Received: April 13, 1999;
Initial review completed: May 18, 1999;
Revision Accepted: August 30, 1999
Velocardiofacial syndrome (VCFS) is a genetic
disorder with an estimated frequency of 1 in 4000 live births(1).
This disorder is characterized by cardiac defects, cleft palate,
learning disabilities and mild facial dysmor-phology(2). The
identification of these patients is difficult because it is a
multisystem syndrome with numerous anomalies, many of which are
considered minor and found in general population(3). The enormous
variability of this condition is seen by the different clinical
features which are present in the affected members of the same
family(4,5). There is a paucity of documentation on this subject
in Indian literature. Hence we report a pair of siblings born to
nonconsanguineous parents who had variable clinical phenotype.
Case Reports
Case 1:
A 7½-year-old boy was referred for
evaluation of developmental delay and abnor-mal behavior. He was
delivered normally at term with an uneventful perinatal period. He
had cleft palate which was repaired at 4 years of age. He had
delay in acquiring milestones in all sectors. The parents reported
poor scholastic performance as well as hypernasality of speech
since he started verbalizing. He had frequent chest infections and
was diagnosed to have a ventricular septal defect at 1 year of
age.
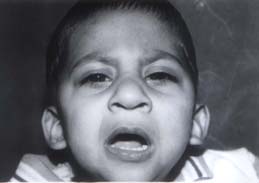
On physical examination the patient was short
statured, [height - 115.6 cm (93% of median)] and had microcephaly
[head circumference 44.3 cm (<3 SD)]. He had a long face with
prominent nasal bridge and a broad tip of the nose. He had flat
maxillae, microg-nathia and retruded mandible with a repaired
cleft palate. The child had an everted upper lip with short
philtrum. The ears were prominent and symmetric (Fig. 1).
He had typical slender hands with tapering fingers which were
hyperextensible (Fig. 2).
On evaluation of intelligence, his IQ was 32.
Social quotient assessment by VSMS scale was 38.6. On
developmental profile, his academic age was 2 years 4 months and
his social age was 3 years 6 months. His behavior pattern was
preservative, stereotypic, and not goal directed.
Chest X-ray revealed cardiomegaly and
echocardiography showed a small perimem-branous ventricular septal
defect. His bone age was normal; computed tomography scan of brain
and ultrasound abdomen for kidneys did not reveal any structural
defects. Ophthalmo-logical assessment and audiometry was normal.
 |

|
|
Fig. 1. Typical facial findings in Case 1
with velocardiofacial syndrome.
|
Fig. 2. Hands of Case 1 showing spindle
shaped and tapering fingers. |
Case 2:
This 1½-year-old male was the
younger brother of Case 1. He was delivered full term of an
uneventful pregnancy and had no birth asphyxia. The child had
feeding difficulties and failure to thrive since birth. There was
history of nasal regurgitation of milk and he also had a cleft
palate which was repaired at 1 year of age. He had developmental
delay in all sectors. The parents complained that the child was
floppy since birth and also had constipation.
On examination he had dysmorphic features. His
length was 72 cm (90% of median) and head circumference was 42.5
cm (<3 SD). He had narrow palpebral fissures, maxillary
deficiency, microsomia, small chin and a large fleshy nose, a
broad nasal bridge with asymmetric prominent auricles (Figs. 3
& 4). Cardiovascular examination was normal. Neurological
assessment revealed gross motor and fine motor and language delay.
The child was hypotonic but reflexes were normally elicitable.
On investigation the echocardiography, CT scan
head, bone age, thyroid profile, serum calcium and ultrasound
abdomen were within normal limits.
Both the children were diagnosed as cases of
velocardiofacial syndrome and they were provided rehabilitation
particularly speech therapy and special education. The parents
were examined in details and were not found to have any features
of the syndrome. The grandparents could not be contacted.
The parents were informed about the variable
penetrance and manifestations of the syndrome and its associated
problems. They were advised to get chromosomal anlaysis including
FISH analysis and to bring the children for periodic follow up.
|
|

|
|
Fig. 3. Facial features of velocardiofacial syndrome in
Case 2.
|
Fig. 4. Lateral view of face of Case 2. |
Discussion
VCFS was initially described by Sphrintzen et
al. in 1978 as a multiple malformation syndrome that included
clefting of palate, cardiac anomalies, a characteristic facial
phenotype and learning disability(6). Since then more than 40
physical anomalies including hypocalcemia, hypotonia, mental
retardation, thrombocytopenia, blood vessel anomalies such as
tortuous retinal vessels have been described(7). A newly
recognized finding is the presence of psychiatric disorder in
these patients(8).
The typical patient with VCFS presents with a
cluster of velar, cardiac, facial, digital and mental findings.
All these features were amply demonstrated in Case 1. The
characteristic facial features found in these cases are a long
vertical face, large fleshy nose, narrow alar base, flattened
malar region, narrow palpebral fissures, retrognathia, small
downturned mouth and prominent ears(6). Both the children had
characteristic facies and were also short statured as is found in
30% of cases(2). A small head circumference which was present in
both the cases is a common finding. Recently, structural brain
defects have been described(9) but they were not present in either
of the cases.
The oral manifestations consist of clefts of
the secondary palate and velopharyngeal insufficiency(10). Both
the brothers had cleft palate which were repaired. The elder sib
had hypernasality of speech, which was probably due to
velopharyngeal insufficiency. The history of feeding difficulties,
failure to thrive and nasal regurgitation of milk in the younger
boy could also be explained by the presence of the oral
manifestations.
These children commonly have motor
incoordination and poor development of numerical concepts. These
along with poor abstract reasoning leads to increasingly poor
psychological, language and academic performance(9). Personality
may tend towards preservative stereotypic behavior as was seen in
Case 1.
The problems with which such children generally
present in infancy were all seen in Case 2, i.e., hypotonia,
development delay, constipation and failure to thrive.
Not all principal features are present in each
case; particularly cardiac disease is not an essential feature.
The elder sib had VSD but the younger sib did not. The younger sib
also did not have typical digital findings like spindle shaped
slender fingers. Frequent upper respira-tory tract infections,
pneumonia or bronchitis are common in VCFS as were reported only
in the elder sib(9). Studies on monozygotic twins and affected
members of the same family who have different clinical features
show the enor-mous variability seen in this conditions(4,5).
In 1993 the New Castle and Tyne group suggested
the acronym CATCH22 as an alternative name for this syndrome [C =
cardiac anomalies, A = abnormal facies, T = thymic hypoplasia, C =
cleft palate, H = hypocalcemia, 22 = affected chromosome](11).
Both hypocalcemia and thymic hypoplasia were absent in both the
cases. Hypothyroidism which has also been described as an
associated finding was absent in these sibs(7). Conductive hearing
loss caused by chronic otitis media found in 77% of the typical
cases was not found in either of the sibs(12).
The identification of this disorder is dificult
because it is a multisystem syndrome with numerous anomalies.
There is no clinical find-ing which is pathognomonic for diagnosis
of VCFS nor is there a composite of major and minor criteria that
can be used to make a definitive diagnosis(3). Therefore it is
important to consider the diagnosis in any patient with more than
one of the clinical findings characteristic of this syndrome.
As more is learned and new clinical findings
are uncovered in patients with VCFS, the spectrum of affected
patients encompasses many patients previously described as having
DiGeorge syndrome (DGS), Pierre Robin Sequences (PRS) and the
CHARGE associa-tion. Both our cased did not have hypocalcemia,
thymic aplasia, short philtrum of lip and anti-mongoloid slant of
eyes which are characteristic of DGS. The pair of brothers did not
have glossoptosis which is one of the three features like cleft
palate and micrognathia which are found in PRS. On the contrary
many other facial features, cardiac findings and skeletal changes
characteristic of VCFS were found in them. These children did not
fit into CHARGE association as there was absence of coloboma in
the eyes, choanal atresia, genital hypoplasia and deafness.
Most cases of VCFS are sporadic, but when
inherited, it has an autosomal dominant pattern of transmission
with variable penetrance. It results from a deletion of 22 q
11.2(13). High resolution Karyotyping and DNA analysis which is
required to pick up the genetic make up of these cases is
advisable.
1. Burn J, Goodship J. Congenital heart
disease. In: Emery and Rimoin’s principles and Practice
of Medical Genetics, 3rd edn. Eds. Rimoin DL, Connor JM, Pyeritz
RE. New York, Churchill Livingstone, pp 767-828.
2. Smith DW. Shprintzen syndrome (Velocardio-facial
syndrome) In: Recognizable Patterns of Human Malformations,
5th edn. Ed. Smith DW. Philadelphia, W.B. Saunders Co; 1997; pp
266-267.
3. Motzkin B, Marlon R, Goldberg R, Shprintzen
R, Saenger P. Variable phenotypes in velocardio-facial syndrome
with chromosomal deletion. J Pediatr 1993; 123: 406-410.
4. Goodship J, Cross I, Scambler P, Burn J.
Monozygotic twins with chromosome 22q 11 deletion and discordant
phenotype. J Med Genet 1995; 32: 746-748.
5. Holder S, Winter R, Kamath S, Scambler P.
Velocardiofacial syndrome in a mother and daughter: Variability of
the clinical phenotype. J Med Genet 1993; 30: 825-827.
6. Shprintzen RJ, Goldberg RB, Lewin ML, Sidoti
EJ, Berkman MD, Argamaso RV, et al. A new syndrome
involving cleft palate, cardiac anomalies, typical facies and
learning disabilities: Velocardiofacial syndrome. Cleft Palate J
1978; 5: 56-62.
7. Goldberg R, Motzkin B, Marion R, Scambler PJ,
Shprintzen RJ. Velocardiofacial syndrome: A review of 120
patients. Am J Med Genet 1993; 45: 313-319.
8. Carlson C, Papolos D, Pandita RK, Faedda GL,
Veit S, Goldberg R, et al. Molecular analysis of velocardio-facial
syndrome patients with psychiatric disorders. Am J Hum Genet 1997;
60: 851-859.
9. Pike AC, Super M. Velocardiofacial syndrome.
Postgrad Med J 1997; 73: 771-775.
10. Finkelstein Y, Zohar Y, Nachmani A, Talmi
YP, Lerner MA, Hauben DJ, et al. The otolaryngologist and
the patient with velocardio-facial syndrome. Arch Otolaryngol Head
Neck Surg 1993; 119: 563-569.
11. Wilson D, Burn J, Scambler P, Goodship J.
Digeorge syndrome part of Catch 22. J Med Genet 1993; 30: 852-856.
12. Shprintzen RJ, Goldberg RB, Young D,
Wolford I. The velocardiofacial syndrome: A clinical and genetic
analysis. Pediatrics 1981; 67: 167-172.
13. Carlson C, Sirotkin H, Pandita R, Goldberg R, McKie J,
Wadey R, et al. Molecular definition of 22q 11 deletions in
151 Velocardiofacial syndrome patients. Am J Hum Genet 1997; 61:
620-629.
|
