|
|
|
Indian Pediatr 2020;57:
266-267 |
 |
Recurrent Peumonia in an Infant With an Esophageal Lung
|
|
Neha thakur1*, Dipti Agarwal1,
Shamrendra Narayan2 and Deepanshu Shukla1
Department of 1Pediatrics and 2Radiodiagnosis,
Dr Ram Manohar Lohia Institute of Medical Sciences, Lucknow,
Uttar Pradesh, India.
Email:
nehaimsbhu@gmail.com
|
|
Esophageal lung is a rare variety of
communicating bronchopulmonary foregut malformation with
anomaolous communication between an isolated portion of
respiratory tissue and esophagus. Children present in early
life with recurrent cough and pneumonia. Majority of the
reported cases are associated with other anomalies like
tracheoesophageal fistula. We report a case of a 7-month-old
girl with right sided esophageal lung who was misdiagnosed
as dextrocardia with right sided pneumonitis.
Keywords: Bronchopulmonary, Dextrocardia,
Lung malformation, Recurrent cough.
|
|
Esophageal lung is a rare communicating bronchopulmonary foregut
malformation with anomalous origin of the main bronchus from the
esophagus usually on the right side, which leads to recurrent aspiration
pneumonitis. Other associated congenital anomalies of the upper
gastro-intestinal tract, ribs and vertebrae may be present. It is
diagnosed radiologically and confirmed by broncho-scopy. Few cases have
so far been reported in literature [1]. A high index of suscpicion
should be kept in young children with recurrent chest infection.
A 7-month-old girl presented with recurrent lower respiratory tract
infection and episodes of choking following breast feeding since one
month of age. She was symptomatic in the present episode for last 7 days
for which she received oral amoxycillin for 5 days without improvement.
The baby was born full term by normal delivery and was developmentally
normal. At admission, child had low weight and length as per age,
tachypnea (respiratory rate 72/minute), tachycardia (heart rate
130/minute) with subcostal and intercostal retractions. On auscultation,
breath sounds were decreased on right side with apex beat on the right
side suggestive of dextrocardia. Hemoglobin was (10g/dL), total
leucocyte count was 27700/µL (neutrophils 74%), C-reactive protein was
positive, with normal renal and liver functions. Blood culture was
sterile. Chest X-ray showed hazy right hemithorax with mediastinal shift
to the right side. Contrast enhanced computed tomographic (CT) scan
thorax demonstrated right lung hypoplasia with cystic bronchiectatic
changes with nonvisualization of right main bronchus, hypoplastic right
main pulmonary artery and abnormal bronchesophageal communi-cation (Fig.
1a, 1b). Barium swallow study showed filling of right main
bronchus directly from the esophagus. Rigid bronchoscopy revealed a
blind ended right bronchial stump which confirmed the diagnosis of
esophageal lung. Ultrasound abdomen and echocardigraphy were normal.
Child improved with oxygen, intravenous antibiotics and nebulisation
with bronchodilators. Child started accepting orally and was gradually
tapered off oxygen. She was advised operative intervention for
esophageal lung (right pneumonectomy with resection of the esophageal
bronchus and repair of the esophagus at the site of bronchial
communication), which the family refused.
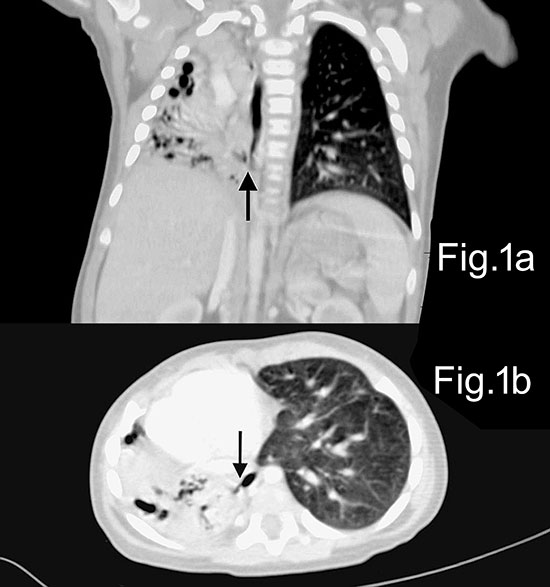 |
| Fig. 1 (a) CT
lung (coronal section) demonstrating right lung
hypoplasia with nonvisualization of right main bronchus
with arrow showing communication of lung with lower
esophagus; (b) axial image with arrow demonstrating
communication of lung with esophagus. |
Congenital bronchopulmonary foregut malformation
comprises of an abnormal patent tract between respiratory and
gastrointestinal tract as a result of anomalous budding of the
embryonic foregut and tracheobronchial tree [2]. It has been
classified into 4 groups [3] viz, group I (16%) with associated
esophageal atresia and tracheoesophageal fistula, group II (33%)
where one lung originates from the lower esophagus (esophageal
lung), group III (46%) with an abnormal communication between an
isolated anatomic lung lobe or segment with the esophagus or
stomach (esophageal bronchus), and group IV (5%) with
communication of normal bronchial system with esophagus.
Patients present with failure to thrive, chronic cough and
recurrent pneumonia. Those with severe anomalies present early
in life with cough on feeding, also known as Ono´s sign [4].
Eosphageal lung is commonly seen in females with a ratio 1.5 to
1 with preferential right lung involvement like index case [5].
This probably results from proximity of the right mainstem
bronchus with the esophagus. Esophageal lung can be associated
with other anomalies of cardiac, respiratory or gastrointestinal
tract. The definitive treatment is surgical correction.
All children with recurrent pneumonitis and cough following
feeds should be thoroughly investigated. The present case was
referred with diagnosis of dextrocardia with pneumonia.
Radiological investigations were suggestive of esophageal lung.
A high index of suspicion and detailed work up should be done in
children with recurrent pneumonia.
Contributors:
NT,DA,DS: case management; SN: radiological investigations. All
the authors were involved in drafting the manuscript reviewing
the literature and approve the final manuscript.
Funding:
None; Competing interest: None stated.
REFERENCES
1. Sugandhi N, Sharma P, Agarwala S, Kabra SK,
Gupta AK, Gupta DK. Esophageal lung: Presentation, management,
and review of literature. J Pediatr Surg. 2011;46:1634-7.
2. Berrocal T, Madrid C, Novo S. Congenital anomalies of the
tracheobronchial tree, lung, and mediastinum: Embryology,
radiology, and pathology. Radiographics. 2004;24:e17.
3.
Srikanth MS, Ford EG, Stanley P, Mahour GH. Communicating
bronchopulmonary foregut malformations: Classification and
embryogenesis. J Pediatr Surg. 1992;27: 732-6.
4. Osinowo
O, Harley HR, Janigan D. Congenital broncho-oesophageal fistula
in the adult. Thorax. 1983;38:138-42.
5. Verma A, Mohan
S, Kathuria M, Baijal SS. Esophageal bronchus: Case report and
review of the literature. Acta Radiol. 2008;49:138-41.
|
|
|
 |
|
