Early diagnosis and targeted therapy are essential
for reducing the burden of neonatal sepsis in terms of mortality and
emerging antibiotic resistance [1]. Blood culture remains the gold
standard for diagnosis of sepsis [2,3]. Non-availability of blood
cultures or false-negative results hamper in provision of
organism-specific antibiotics. Blood culture in neonatal period faces
challenges of diagnostic accuracy owing to use of intrapartum
antibiotics, use of prior antibiotics in referring hospitals, and growth
of organisms with low colony counts [3].
Various methods have been tried to enhance the yield
of blood cultures. These include inoculation of high volume of blood
into culture bottles, automated continuous blood culture monitoring
systems and use of 2 or more blood cultures, maintaining blood-broth
ratio of 1:5 to 1:10 and avoiding samples from indwelling catheters for
risk of contamination [4-6]. In developing countries, the lack of good
antenatal care, sub-standard hospital care and irrational antibiotic
usage might affect the culture positivity rates. We could not find any
published data from India or any other developing country on the
efficacy of two blood cultures in enhancing the isolation rates of
organisms in suspected neonatal sepsis.
We designed this prospective cohort study to evaluate
the increase in culture positivity rate by taking two blood cultures
drawn during the same time frame.
Methods
This study was a prospective cohort study conducted
at the Neonatal division of Department of Pediatrics of a tertiary-care
institute from August 2014 to July 2015. The study was approved by the
institutional ethics committee.
All neonates >30 weeks of gestation admitted to the
unit till 28 days of life were evaluated for sepsis. Criteria for
inclusion were presence of at least one clinical feature with two or
more risk-factors for sepsis. Risk factors considered were prolonged
rupture of membranes (>24 hours prior to delivery), foul smelling liqor,
maternal fever (temperature >100.4ºF) within 2 weeks of delivery or
during labor, prolonged labor (>24hr), multiple vaginal examinations (>3
sterile or single unclean per vaginal examination), dai handling,
delayed cry (>5min in extramural births or APGAR score <4 at 1 min in
intramural births) and prematurity (<37 completed weeks), previous
hospital stay and history of faulty feeding in the form of bottle
feeding or use of diluted animal milk. The clinical indicators of sepsis
were respiratory distress, refusal to feed, abdominal distension,
regurgitation, loose stools, hypothermia, fever, lethargy and bleeding,
in absence of any other identifiable cause. Exclusion criteria were
patients who had received antibiotics before blood culture sampling (Fig.
1). Neonates included in the study underwent standard sepsis screen.
Blood cultures were taken after cleansing the skin site with 70%
isopropyl alcohol for 30 seconds followed by 1-2% tincture iodine and
isopropyl alcohol again. The usual time between two cultures was about
5-8 minutes but never more than 15 minutes. 1 mL blood samples were
drawn separately from two peripheral veins and inoculated into BactT/Alert
(Paed Plus) bottles. The cultures were observed for 5 days before
reporting as negative. Identification of bacteria and antibiotic
sensitivity testing was done by standard bacterial methods as per the
CLSI guidelines [7]. All Gram negative pathogens and S. aureus
were considered true positive even if isolated in any one of the blood
cultures. Isolation of CONS and Candida spp. in only one of the
cultures was considered true culture positive only with positive sepsis
screen. If two or more of the following parameters were positive, it was
considered a positive sepsis screen: (i) Total leukocyte count
<5000/cumm; (ii) Absolute neutrophil count: Low counts (as per
Manroe chart for term and Mouzinho’s chart for VLBW infants); (iii)
Immature/total neutrophil >0.2; 4) Micro-ESR >15 mm in 1st hour; 5) C
reactive protein >10 mg/l and clinical course consistent with
sepsis. Candida spp. or CONS grown in both cultures were considered true
culture positives. Only one of the cultures positive for CONS or
Candida, with normal sepsis screen or clinical course not suggestive of
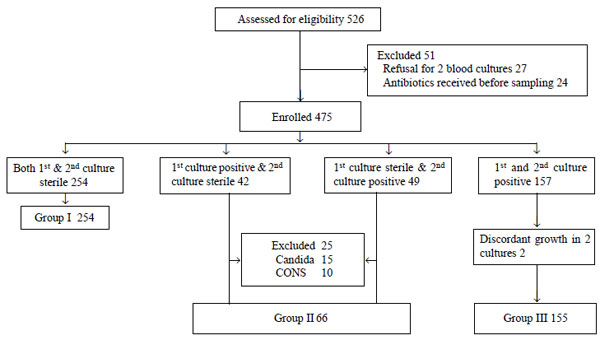
sepsis, was defined as contaminant. The study participants were divided
into 3 groups i.e. Group I (both cultures sterile), Group II
(either culture positive) and Group III (both cultures positive) and
their outcomes were compared (Fig. 1).
 |
|
Fig. 1 Flowchart showing study
participants.
|
A pre-designed proforma was used to gather data and
patients were enrolled after taking informed written consent of the
parents. The neonates were evaluated for the course of the disease and
complications like pneumonia, meningitis, acute renal failure, bleeding,
sclerema and death.
Primary objective of this study was diagnosis of
extra cases of culture-proven sepsis with the use of two blood cultures.
Our secondary objectives included comparison of clinical outcomes in the
three groups, determination of common pathogenic organisms, and
diagnosis of contaminants in blood culture.
In the year prior to start of this study, the culture
positivity rate with use of one blood culture was 30%. In a pilot study
run over one month in our unit, the overall culture positivity was 40%
with double blood culture method. To increase the culture positivity
from 30% to 40%, with risk difference of 0.1 and 2-tailed p value of 90,
the estimated sample size was calculated to be 475, at an alpha error of
5%.
Statistical analysis: Statistical analysis
was done using Stata 12 software. Continuous variables were analyzed
using t test, ANOVA/Kruskal Wallis test and multiple comparisons were
done using Bonferonni adjustment. Categorical variables were analyzed
using chi-square/ Fisher’s exact test.
Results
There were 526 patients admitted with an initial
diagnosis of suspected sepsis, of which 475 neonates were enrolled (Fig
1). The mean (SD) gestational age was 35.1 (2.4) weeks and mean (SD)
birth weight was 2.1 (0.58) kg. The median age of neonates at admission
was 72 (range 1-696) hours. The most common presenting complaints were
respiratory distress, poor feeding, lethargy and hypothermia.
First blood culture positive was seen in 185 cases
(38.9% first culture positivity rate). When we added the second culture
positivity, the yield increased to 221 (46.5% total culture positivity
rate). The increase in culture yield was 36 (7.6%), with 95% CI of 2.41
to 12.79, (P= 0.018). Those with culture positivity had a
significantly higher proportion of positive sepsis screen (45.2%)
compared to those with both culture sterile (29.5%).
E. coli. was the most common organism isolated.
E. coli and Candida spp.were the most common organisms
responsible for early and late onset sepsis, respectively. None of the
cultures showed polymicrobial growth. On initial evaluation, there were
91 patients in group II and 155 in group III. In group II (only one of
the two cultures positive), there was growth of E. coli in 16,
K. pneumoniae in 10, S. aureus in 38, Candida in 17
and CONS in 10 babies. Among 17 babies with Candida and 10 with
CONS, only 2 with Candida growth were considered true culture
positive. Other 25 babies (15 with candida and 10 with CONS) had
negative sepsis screen and clinical course not consistent with sepsis,
and were considered as contaminats.
There were two patients with discordant results: one
with CONS and Candida spp. and the other with CONS and Klebsiella
in first and second blood culture, respectively. The former was
discarded as contaminant and the latter was counted as Klebsiella-positive
under group II. The details of organisms isolated in the cultures is
provided in Table I.
TABLE I Distribution of Organisms in Blood Culture Samples
|
Organism |
Isolated |
Discarded |
Included |
Isolated |
Discarded |
Included |
Group III* |
Different |
|
isolated |
only in 1st |
as conta- |
in |
only in 2nd |
as conta- |
in |
|
organisms |
|
culture |
minant |
Group II* |
culture |
minant |
Group II* |
|
in two |
|
|
|
|
|
|
|
|
cultures |
|
Escherichia coli (n=63) |
8 |
0 |
8 |
8 |
0 |
8 |
47 |
0 |
|
Klebsiella pneumonia (n=38) |
4 |
0 |
4 |
6 |
0 |
6 |
28 |
1 |
|
Pseudomonas aerugi- nosa (n=2) |
0 |
0 |
0 |
0 |
0 |
0 |
2 |
0 |
|
Acenitobacter baumannii (n=2) |
0 |
0 |
0 |
0 |
0 |
0 |
2 |
0 |
|
Staphylococcus aureus (n=56) |
17 |
0 |
17 |
21 |
0 |
21 |
18 |
0 |
|
CONS** (n=8) |
6† |
6 |
0 |
4† |
4 |
0 |
8 |
2 |
|
Candida sps (n=52) |
7† |
7 |
0 |
10‡ |
8 |
2 |
50 |
1 |
|
**Coagulase negative Staphylococcus, †All discarded as
contaminants, ‡8 discarded as contaminants; *Group I- Culture
negative patients, Group II- Single blood culture positive,
Group III- Both cultures positive. |
There were significantly more LBW babies (74%) and
preterms (49%) in the culture-positive group than in Group I (59% and
24%, respectively). Major morbidities and mortality were more common in
blood culture-positive patients (Group II or Group III) as compared to
culture-negative babies in Group I. However, there was no significant
difference between Group II and Group III (Table II).
TABLE II Outcomes in Blood Culture Positive and Negative Groups
| |
Group (%) |
P values |
|
Morbidities/outcome |
I*(n=254) |
II*(n=66) |
III* (n=155) |
I vs II |
I vs III |
II vs III |
|
Pneumonia (n= 54) |
10(4) |
11(16.7) |
33(21) |
<0.001 |
<0.001 |
0.431 |
|
Meningitis (n=32) |
0/77(0) |
12/44(27) |
20/82(24.4) |
<0.001 |
<0.001 |
0.723 |
|
Bleeding (n=86) |
24(9.5) |
19(29) |
43(27.7) |
<0.001 |
<0.001 |
0.874 |
|
Acute renal failure (n=12) |
3(1.2) |
3(4.5) |
6(4) |
0.073 |
0.072 |
0.816 |
|
Sclerema (n=7) |
0(0) |
2(3) |
5(3) |
0.005 |
0.004 |
0.939 |
|
NEC (n=12) |
0(0) |
3(4.5) |
9(6) |
0.049 |
0.026 |
0.830 |
|
Thrombocytopenia (n=166) |
54(21) |
31(47) |
81(52) |
<0.001 |
<0.001 |
0.472 |
|
Mortality (n=128) |
44(17) |
20(30) |
64(41) |
0.019 |
<0.001 |
0.124 |
|
*Group I- Culture negative patients, Group II- Single blood
culture positive, Group III- Both cultures positive. |
Discussion
It was observed in the present study that taking two
blood cultures increased the culture yield by 7.6%. Major morbidities
were comparable in babies with either one or both cultures positive but
they were more than in babies with both cultures sterile.
Previous studies on culture positivity in neonates
have reported an isolation rate ranging from 25-60% [8–10]. Although few
studies have reported lower culture positivity rates but it could be due
to low blood volume taken for culture or administration of antibiotic
before blood collection [11,12].
Wiswell, et al. [13] were among the first to
document advantage of two site blood cultures in initial evaluation of
neonatal sepsis. They had taken 2 sets of blood cultures (1 aerobic and
1 anerobic) from different sites in 460 inborn infants during 1st week
of life. In 8 neonates, bacteremia was confirmed while in 10 cases,
contamination from skin flora was documented. This was a retrospective
study and included neonates upto first week of life only.
Sarkar, et al. [14], in a prospective study
had taken blood cultures from two different peripheral sites 15- 30
minutes of each other in 216 neonates with suspected sepsis. In their
study, 20 (9.2%) of 216 neonates had 22 episodes of culture-proven
sepsis. All neonates with positive cultures grew the same organism with
a similar sensitivity pattern from the two different peripheral sites.
The remaining 196 neonates had negative blood cultures from both the
sites. They did not document any advantage of double site cultures in
detection of neonatal septicemia. The difference in results from the
present study could be due to smaller sample size and inclusion of only
inborn neonates.
CONS and Candida spp. are frequently isolated
organisms in neonates admitted in neonatal intensive care units [15]. As
these organisms form part of the skin flora, they can be mere
contaminants in a blood culture growth if the skin is not prepared well
before taking culture [16–18]. Struthers, et al. [19] conducted a
prospective study with the objective of differentiating pathogenic from
contaminant CONS and reducing antibiotic usage. One hundred pairs of
cultures were drawn from two percutaneous sites from 69 babies with
suspected sepsis after 48 hours of life. They also considered one
positive culture of CONS as contaminant and both positive cultures as
infection. They differentiated between contaminant CONS in 5 neonates
who had growth in one of the two cultures only and pathogenic CONS in 16
neonates with both positive cultures. In contrast, the present study had
a significant proportion of isolates which were reported as
contaminants.
The strength of the study is its prospective design,
large sample size, a representative sample including extramural babies
with both early and late neonatal sepsis. Limitations of our study were
that colony count and time to positivity could not be documented.
It is concluded that two simultaneous blood cultures
significantly increased culture positivity in neonates with sepsis. This
could be useful in referral neonatal units where the admission rates for
babies with sepsis are high. As the overall incidence of CONS and fungal
sepsis is on an upsurge, the policy of two blood cultures can be helpful
to rule out contamination in units with high rates of these organisms.


