A 7-year-old boy was brought to us with swelling of the
right knee since 1 year of age. The swelling used to appear
suddenly once every two months, would last for a few days
and then gradually subside on its own. During the episode,
the patient used to have severe pain in the knee joint and
was not able to walk. There were no aggravating or relieving
factors. There was no history of fever, trauma, bleeding
from any other site or swelling of any other joint.
Examination revealed a child with a
fluctuating, tender swelling on the medial aspect of the
right knee joint (Fig. 1). Movements at the
right knee joint were restricted. Further examination
revealed a swelling on the medial aspect of the right foot,
just in front of medial malleolus, fluctuant, non-tender,
which used to decrease in size on raising the leg and used
to blanch on pressure. The parents informed that this
swelling was present since birth. Careful scrutiny also
revealed that the affected limb was clearly hypertrophied
and larger than the unaffected limb.
 |
|
Fig.1. Right-sided
hemarthrosis
|
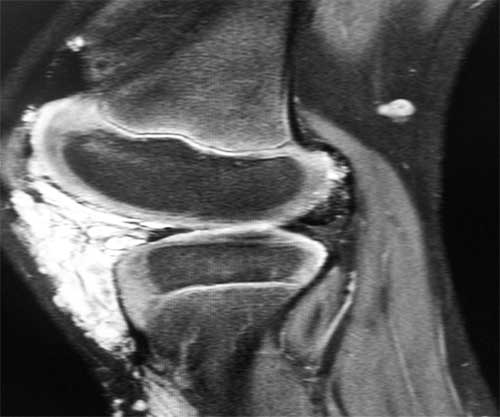
An MRI of the right lower limb was
suggestive of a diffusely insinuating vascular malformation,
haemolymphatic in nature, noted along the antero-medial
aspect of the right leg with intra-articular extension and
distension of the knee joint with mild joint effusion and
evidence of intra-articular hemorrhage due to prior bleeds (Fig.
2). Similar focal lesions were also noted on the dorsum
and medial aspect of the foot. The vascular surgeon plans to
thrombose the vascular supply of the intra-articular portion
of the malformation to prevent the recurrent hemarthrosis
which would otherwise eventually destroy the joint.
 |
|
Fig.2. Intra-articular
bleed
|
Klippel Trenaunay syndrome is a cutaneous
vascular malformation that, in combination with bony and
soft tissue hypertrophy and venous abnormalities,
constitutes the triad of defects of this usually
nonheritable disorder [1]. However, interestingly, scattered
reports are available in world literature that it may
occasionally be inherited [2,3]. Our child had asymmetric
limb hypertrophy, vascular malformations as well as a
cutaneous vascular malformation on the lower foot. The lower
limb is involved in 95% of the cases [4]. While bleeding
from the vascular lesions are infrequent complications (hematuria
from a vascular malformation of the urinary tract or rectal
bleeding from a gut lesion) [4], intra-articular bleeds from
such a lesion are extremely rare [5]. Screening of this
child revealed no other associated features such as
lymphatic obstruction, spina bifida, hypospadias,
polydactyly, syndactyly, oligodactyly, orofacial
abnormalities, hyperhidrosis, hypertrichosis, paresthesia,
or decalcification of bones [4].
1. Cohen M. Klippel-Trenaunay syndrome.
Am J Med Genet. 2000;93:171-2.
2. Ceballos-Quintal JM, Pinto-Escalante
D, Castillo-Zapata I. A new case of Klippel-Trenaunay-Weber
(KTW) syndrome: evidence of autosomal dominant inheritance.
Am J Med Genet. 1996;63:426-7.
3. Hofer T, Frank J, Itin PH.
Klippel-Trenaunay syndrome in a monozygotic male twin:
supportive evidence for the concept of paradominant
inheritance. Eur J Dermatol. 2005;15:341-3.
4. Jones K. Smith’s Recognizable Patterns
of Human Malformations. 6th ed; Philadelphia,
Elsevier Saunders: 2009.p.598-9.
5. Catre M, Kolin A, James P, Waddell J. Total knee
arthroplasty in Klippel-Trenaunay syndrome Can J Surg.
2005;48:494-5.


