|
|
|
Indian Pediatr 2011;48: 233-235 |
 |
Percutaneous Transluminal Coronary Angioplasty
Following Kawasaki Disease |
|
Vikas Kohli, MS Sachdev and Vipul Roy
From Pediatric Cardiology and Congenital Cardiac Surgery
Unit, Indraprastha Apollo Hospital, New Delhi, India.
Correspondence to: Dr Vikas Kohli, C-116 Sarita Vihar,
New Delhi 110 044, India.
Email: [email protected]
Received: June 12, 2009;
Review: July 24, 2009;
Accepted: October 6, 2009.
|
Kawasaki disease (KD) can result in coronary artery disease in the form
of ectasia, aneurysm and stenosis. The final complication can be
myocardial infarction. We report a child who presented with severe left
ventricular dysfunction following KD and was detected on angiography to
have total left anterior descending artery occlusion. Angioplasty was
done which resulted in improvement in the flow. Follow up angiography a
year later showed recurrence of total occlusion.
Key words: Angioplasty, Child, Coronary artery disease,
Kawasaki disease.
|
|
Kawasaki disease (KD) is known to
involve the coronary arteries in upto 20% of patients. Usually acute
involvement is in the form of ectasia or aneurysm formation of the
coronary artery [1,2]. Four percent of all cases may progress to ischemic
heart disease [2]. We report a young child presenting subacutely following
KD, with cardiac dysfunction and complete coronary occlusion. The child
underwent coronary angiography and angioplasty.
Case Report
A 3 year 11 month old male child presented to us with
signs and symptoms suggestive of congestive heart failure for the
preceding one week. He had history of febrile illness 2 months prior to
presentation, the exact cause of which was not diagnosed. He had peeling
of skin on the sole of his feet and his reports revealed platelet count of
800,000/cu.mm during the illness. Creatinine phosphokinase and troponin I
were normal. The electrocardiogram was suggestive of old anterolateral
myocardial infarction with deep Q waves in lead I, aVL, and V 1-
V4. Echocardiogram showed aneurysmal proximal left main coronary artery
and a normal right coronary artery. The left anterior descending (LAD)
could not be delineated. The left ventricle (LV) was dilated and the
interventricular septum was dyskinetic. The ejection fraction was 35%. Two
clots were seen in the apex of left ventricular cavity. Intravenous
heparin was started after admission and the child was discharged few days
later on warfarin and clopidogrel. Echocardiogram a week later showed
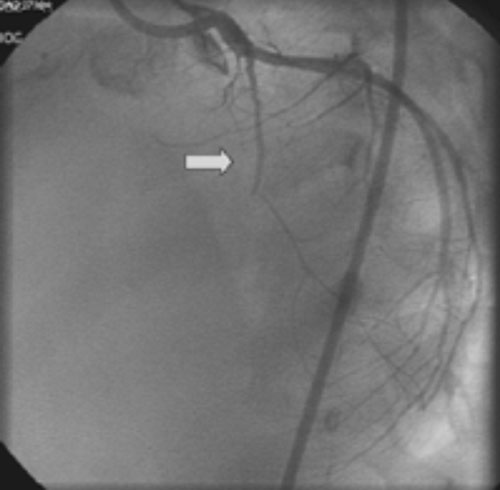
resolution of the LV clots. The child was then taken up for coronary
angiography which revealed an aneurysm in the left main coronary artery
and a complete occlusion of left anterior descending coronary artery (Fig.
1). The percutaneous transluminal coronary angioplasty was
performed 6 weeks later. Following the balloon angioplasty, angiogram
revealed luminal flow into the thin left anterior descending coronary
artery till the level of the 2nd diagonal branch. The patient tolerated
the procedure well and recovered without co-morbidity. He was continued on
warfarin and clopidogrel. He was followed up at 3, 6 and 12 months
following the angioplasty. His echocardiogram at 1 year follow up showed
improved left ventricular function with ejection fraction of 45%. Repeat
angiogram one year after the angioplasty showed total re-occlusion of the
LAD. Clinically the child is in New York Heart Association classification
II.
 |
|
Fig. 1 Selective Left main coronary artery angiogram showing
total occlusion of the Left anterior descending coronary artery.
|
Discussion
The index patient presented to us in congestive heart
failure and an ECG suggestive of anterolateral myocardial infarction. The
past history and investigations were suggestive of a diagnosis of KD.
The fate of coronary artery aneurysm in KD has been
linked to its size [1,2] incidence of coronary artery stenosis in all
cases of aneurysm in KD varies from 19-74% [2,4,5]. The indications of
intervention in KD patients have been previously described [6]. We were
dealing with total coronary occlusion; a less common lesion in KD. Surgery
or percutaneous transluminal coronary angioplasty (PTCA) both were likely
to be associated with re-occlusion. Treatment options for KD related
coronary disease include PTCA, rotational ablation, stenting or coronary
artery bypass grafting.
PTCA may be more effective if performed in younger
patients and early in disease process [7]. Ino, et al. [8]
showed that the effectiveness of PTCA depends on the time interval between
disease onset and treatment, and age of the patient. They suggested PTCA
to be performed in patients younger than 6 to 8 years of age in view of
specific histopathologic features of the disease [8]. A shorter time
interval from KD onset and catheter intervention in successful cases
compared with unsuccessful cases was shown in a report by Japanese
Pediatric Interventional Cardiology Investigation Group [6]. In the
described patient, coronary angioplasty was the chosen method in view of
the child’s age and vessel size and presentation within 2 months of the
disease onset.
PTCA may be associated with a high success rate, but
new aneurysm formation rate is higher than stent implantation or
rotational atherectomy. The etiology of new aneurysms is probably intimal
dissection caused by balloon angioplasty [3]. The incidence of restenosis
after PTCA is high. Approximately one quarter of the patients develop
restenosis or occlusion as happened in our patients [9]. The mechanism
responsible for restenosis is the same as that responsible for failure of
adequate balloon dilation. Coronary arteries with thick intimal
hyperplasia probably recoil easily, even if dilated adequately.
Angioplasty for KD associated coronary disease has recently been reported
in several young children including as young as 2 years old [9]. These
authors have reported medium term patency with angioplasty.
The long term prognosis of MI is not good and there is
likelihood of more areas of stenosis leading to myocardial infarction. 16%
of the survivors from the first attack had a second attack. Fatality was
63% for the second attack and 83% for the third [10]. Our current
objective of management of this patient is to avoid recurrence of
myocardial infarction and optimization of medical management of heart
failure. Since myocardial muscle has already infracted, the patient is
unlikely to benefit from future bypass grafting.
Contributors: VK: Review of first write up
and revisions, editing; MSS: Collection of data, references, first write
up, corrections, review of literature; and VR: Correction of write ups.
Funding: None.
Competing Interest: None stated.
References
1. Kato H, Ichinose E, Yoshioka F, Takechi T, Matsunaga
S, Suzuki K, et al. Fate of Coronary aneurysm in Kawasaki disease:
Serial coronary angiography and long term follow up study. Am J Cardiol.
1982;49:1758-66.
2. Kato H, Sugimara T, Akagi T, Sato N, Hashino K,
Maeno Y, et al. Long term consequences of Kawasaki disease: a 10 to
21 year follow up study of 594 patients. Circulation. 1996;94:1379-85.
3. Akagi T. Interventions in Kawasaki disease. Pediatr
Cardiol. 2005;26:206-12.
4. Onouchi Z, Hamaoka K, Kamiya Y, Hayashi S, Ohmochi
Y, Sakata K, et al. Transformation of Coronary artery aneurysm to
obstructive lesion and the role of collateral vessels in myocardial
perfusion in patients with Kawasaki disease. J Am Coll Cardiol.
1993;21:158-62.
5. Tsuda E, Kamiya T, Ono Y, Kimura K, Kurosaki K,
Echigo S. Incidence of stenotic lesions predicted by acute phase changes
in coronary arterial diameter during kawasaki disease. Pediatr Cardiol.
2005;26:73-9.
6. Akagi T, Ogawa S, Ino T, Iwasa M, Echigo S, Kishida
K, et al. Catheter interventional treatment in Kawasaki disease: a
report from the Japanese pediatric interventional cardiology investigation
group. J Pediatr. 2000;137:181-6.
7. Kuramochi Y, Ohkubo T, Takechi N, Ogawa S.
Feasibility of percutaneous transluminal coronary angioplasty to patients
with kawasaki disease as an early management strategy. Pediatr Cardiol.
2001;22:183-7.
8. Ino T, Akimoto K, Ohkubo M, Nishimoto K, Yabuta K,
Takaya J, et al. Application of percutaneous transluminal coronary
angioplasty to coronary arterial stenosis in kawasaki disease.
Circulation. 1996;93:1709-5.
9. Tsuda E, Miyazaki S, Takamuro M, Fuse S, Tsuji
Y, Echigo S. Strategy for localized stenosis caused by Kawasaki disease:
midterm results of percutaneous transluminal coronary balloon angioplasty
in two infants. Pediatr Cardiol. 2006;27:272-5.
10. Kato H, Ichinose E, Kawasaki T. Myocardial
infarction in Kawasaki disease: clinical analyses in 195 cases. J Pediatr.
1986;108:923-7.
|
|
|
 |
|
