|
|
Research Papers Indian Pediatrics 2007; 44:199-203 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Efficacy of Breast Milk Gastric Lavage in Preterm Neonates |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Archana B. Patel and Samiuddin Shaikh From the Department of Pediatrics and Clinical
Epidemiology Unit, Indira Gandhi Medical College, Correspondence to: Dr. Samiuddin Shaikh, Medha Bhavan,
35 Central Avenue, Nagpur 440 018, Manuscript received: October 3, 2005; Initial review
completed: November 23, 2005;
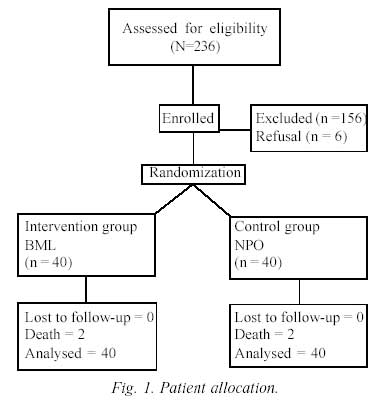
Despite the positive impacts of minimal enteral nutrition (MEN) most practitioners are still in dilemma when and whether to initiate it in sick preterm babies. In practice, MEN is often deferred in preterm having significant perinatal hypoxia, hemodynamic instability, sepsis, abdominal distention, large or bilious gastric aspirate and gastric bleeding(1). Unresolved issues are how soon, how frequent and how much breast milk will provide what benefits to these sick preterm, otherwise commonly managed in most nurseries on exclusive parenteral fluids. We devised a cautious strategy of using at least a gastric lavage with mother’s breast’ milk 4 hours after birth and every 3 hours subsequently till tolerance of nutritive enteral feeds. This could also be used in babies who had gastric bleeding. The study objectives were to evaluate the effects of this gastric lavage in sick preterm babies, on the number of days on parenteral fluids before starting nutritive enteral feeds, duration of hospital stay, morbidity (complications) and mortality. Subjects and Methods This was a prospective open labeled hospital based randomized controlled trial conducted in special care neonatal unit (SCNU) of Indira Gandhi Medical College, Nagpur, India. Babies aged less than 4 hours requiring admission in SCNU and recommended exclusive parenteral fluids by treating physician, were recruited into this study if their birth weight was <1.75 kg and gestation <36 weeks. Babies with congenital anomalies requiring immediate surgical intervention and/or were critically sick in need of assistant ventilation at the time of admission were excluded. Informed parental consent was obtained before entry into the study and the protocol was approved by institutional ethical committee. Outcome variables The main outcome was the mean number of days of exclusive parenteral fluids till successful tolerance of nutritive enteral feeds. Other secondary outcomes were mean length of hospital stay, rate of new complications (shock, sepsis, necrotizing enterocolitis, intracranial hemorr-hage), and mortality. Standard definitions were used to diagnose complications. The babies were categorized as (i) "Improved babies" if they had complication/s or unstable on admission and improved later on, or (ii) "Deteriorated babies" if they had complication/s on admission and subsequently developed another new complication, or, were stable on admission and developed new complications or instability. Sample size estimation The sample size was calculated for the main outcome of mean number of days on parenteral fluids till successful tolerance of nutritive enteral fluids. The assumptions were that the mean days in BPL would be 4 (SD 2) and that in control would be 6 (SD 4). For a 2 sided alpha of 0.05 and power of 0.8 with equal allocation, the total number would be 80 i.e. 40 in each group. Randomization Enrolled babies were randomized into intervention and control group using a computerized random number generator in commuted blocks of 4-6. Baseline assessment This included the birth weight, gestational age, gender, clinical diagnosis and the presence or absence of confounding conditions at admission (perinatal hypoxia, respiratory distress syndrome, shock) and laboratory parameters (hemoglobin, C reactive protein, blood culture, immature/total neutrophil count ratio, gastric lavage for organism and culture). The gestational age was measured using the Ballard’s scoring system(2). Intervention Enrolled babies were randomized into two groups: the intervention or breast milk lavage (BML group) and the control or nil per orally (NPO) group. The BML group received gastric lavage with 5 cc of its own mother’s milk (EBM) within 4 hours of birth and subsequently 3 hourly, through No. 5F nasogastric tube. EBM was left in stomach for 15 minutes and residual was aspirated out. If the aspirate was more than 5 mL then the excess amount was replaced parenterally. This was continued till the treating physician decided to initiate the nutritive enteral feeds. The control group remained "Nil per Oral" or NPO and on exclusive parenteral fluids till the same treating physician decided to start the nutritive enteral feeds. For both groups, the daily fluid requirement was also provided parenterally, till enteral feeds were sufficient to provide the daily fluid and caloric requirement. The decision to initiate nutritive enteral feeds was by the treating physician and not by the study investigators. It was started when baby was hemodynamically stable and had no evidence of shock, clinical sepsis, respiratory distress, abdominal distention, absent bowel sounds, gastric bleeding or bilious aspirate. In both groups, nutritive enteral feeds were termed as successful when three consecutive feeds of 3 mL/kg/feed were tolerated well (i.e., absent of abdominal distention or increase in abdominal girth more than 2 cm from baseline and pre feed gastric aspirate less than 25% of previous feed volume). Gastric lavage with EBM was continued during that period for the intervention group. All babies were nursed under servo controlled open care system. Serum electrolytes were monitored at least once daily during period of gastric lavage. Data analysis Univariate chi-square tests for dichotomous variables and student’s t-test for continuous variables were used. Results A total of 236 newborns were screened and 80 babies were found to be eligible. Figure 1 and Table I show baseline characteristics of both groups. At baseline, the two groups were comparable for all variables except that the BML group had significantly higher number of babies who had presence of some complication (92.5%) as compared to NPO group (70%) (P = 0.009). RDS was the commonest complication present on admission in both groups. Table II shows the univariate differences outcomes between the two groups. In the NPO group 19 (47%) received parenteral fluids for longer than 5 days compared to 7 (17%) of BML (P = 0.004). Hospital stay longer than 3 weeks was in 60% in NPO compared to 30% in BML group.
Table I Baseline Characteristics in BML and NPO Groups
On admission 37 and 28 babies had some complication in BML and NPO group respectively. Of these 18/37 (48.6%) in BML versus 8/28 (28.5%) in NPO "improved", and, 20/40 (50%) in BML versus 27/40 (67.5%) in NPO groups "deteriorated". These were clinically important protective differences with tendency for statistical significance (P = 0.1). Sepsis was the commonest complication observed during hospital stay. Its incidence was lower by 44% in the BML group (30% in BML, 55% in NPO group; RR 0 .58, 95% CI 0.35-0.97; P = 0.02). Four babies died. TABLE II Comparison of the Two Groups for Different Outcomes
* Hyperbilirubinemia requiring exchange transfusion; ** All 4 due to RDS; # Two due to sepsis and 2 because of RDS. Discussion There has been a recent shift in neonatal practice toward the greater and early use of enteral feeds in ill preterm neonates(3). The effects of early introduction of MEN with different types of initial feeds (water, diluted or full strength formulae or breast milk) have been examined in several prospective controlled trials. They showed that early feeding improved intestinal function by preventing gut atrophy without adverse effects(4-9). Our study also contributed to this knowledge base by showing that 3 hourly lavage with 5 cc of breast milk, starting as early as 4 hours after birth resulted in measurable benefits, specifically in reducing the risk of sepsis. Despite emerging evidence on benefits of MEN, many practitioners are skeptical and prefer to withhold it in presence of hemodynamic instability, sepsis, abdominal distention, significant or bilious gastric aspirate and gastric bleeding(1,10). At least a lavage using mother’s milk early after birth, appeared to be the right compromise. It is a cautious balance between withholding enteral feeds and MEN. It also helps neonates with gastric bleeding. Although there were sicker babies in the intervention group at baseline, breast milk lavage lowered the mean number of days on parenteral fluids, mean duration of hospital stay, rate of complications and specifically of sepsis, without increasing risk of necrotizing enterocolitis (NEC). The number of days on parenteral fluids in the BML group was 28% less, the hospital stay 35% less with 44% reduction in sepsis and 26% reduction in other new complications. The reduced number of days on parenteral fluids till successful tolerance of nutritive enteral feeds and reduced hospital stay in the intervention group could be attributed to greater number of "improved" and lesser number of "deteriorated" babies after intervention. In the BML group the relative risk for development of any new complications was 0.61 (95% CI 0.40-0.93). It was significantly lower due to lesser incidence of sepsis (BML = 30%, NPO = 55%, P = 0.02). The mean length of stay in the hospital was reduced by 44% and only 12 i.e. half the number of babies stayed longer than 20 days in BMI group as compared to 24 babies in the NPO group. This protection against infection is attributable to immunologic and antimicrobial properties of breast milk and also supports the hypothesis that gut is often portal of entry in neonatal sepsis(11). Similar results of lowered rate of sepsis have been shown in studies that have used early MEN or early feeding by breast milk(3,12,13). Lavage can also contribute by reducing adhesion of bacteria to the gut mucosa by virtue of presence of an array of oligosaccharide and glycoconjugates in breast milk thereby decreasing their entry in to the circulation(14). It also has the potential to prevent gastric bleeding, promote early resolution of an inflamed mucosa, protect against mucosal per-meability and entry of organisms from inflamed gastric mucosa due to the anti-inflammatory properties of breast milk used for lavage. This shows that gastric bleeds need not be a deterrent to introduction of breast milk. On the contrary lavage with breast milk could assist recovery. The presence of milk in stomach may also stimulate release of enteral hormones particularly gastrin which has trophic effect on gastrointestinal tract thereby improving feeding tolerance later(7). Minimal amount breast milk used for lavage could also provide bioactive and growth factors which improve weight gain and early discharge. There was no difference in overall mortality in the two groups. There were 4 deaths in each group. However, two in the NPO were due to sepsis whereas all 4 in BML were due to RDS of prematurity, which was in higher proportion even at baseline. There are concerns about early introduction and lavage with breast milk. Only one baby developed NEC in the NPO group. So, in this study this concern was alleviated as it was seen in the control group. Thus, in conclusion this study showed that breast milk can safely be introduced to sick preterms. They can be substantially benefited by an early and frequent exposure to the mother’s milk using a simple procedure of gastric lavage even in presence of gastric bleeds. Once the baby stabilizes MEN can be introduced. This can be used in primary care setting as well. Contributors: Both authors were involved in concept, design, data collection, analysis and drafting of the manuscript. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()