|
|
Original Article Indian Pediatrics 2006; 43:210-216 |
||||||||||
|
Incidence of Periventricular Leucomalacia Among a Cohort of Very Low Birth Weight Neonates (<1500 g) |
||||||||||
|
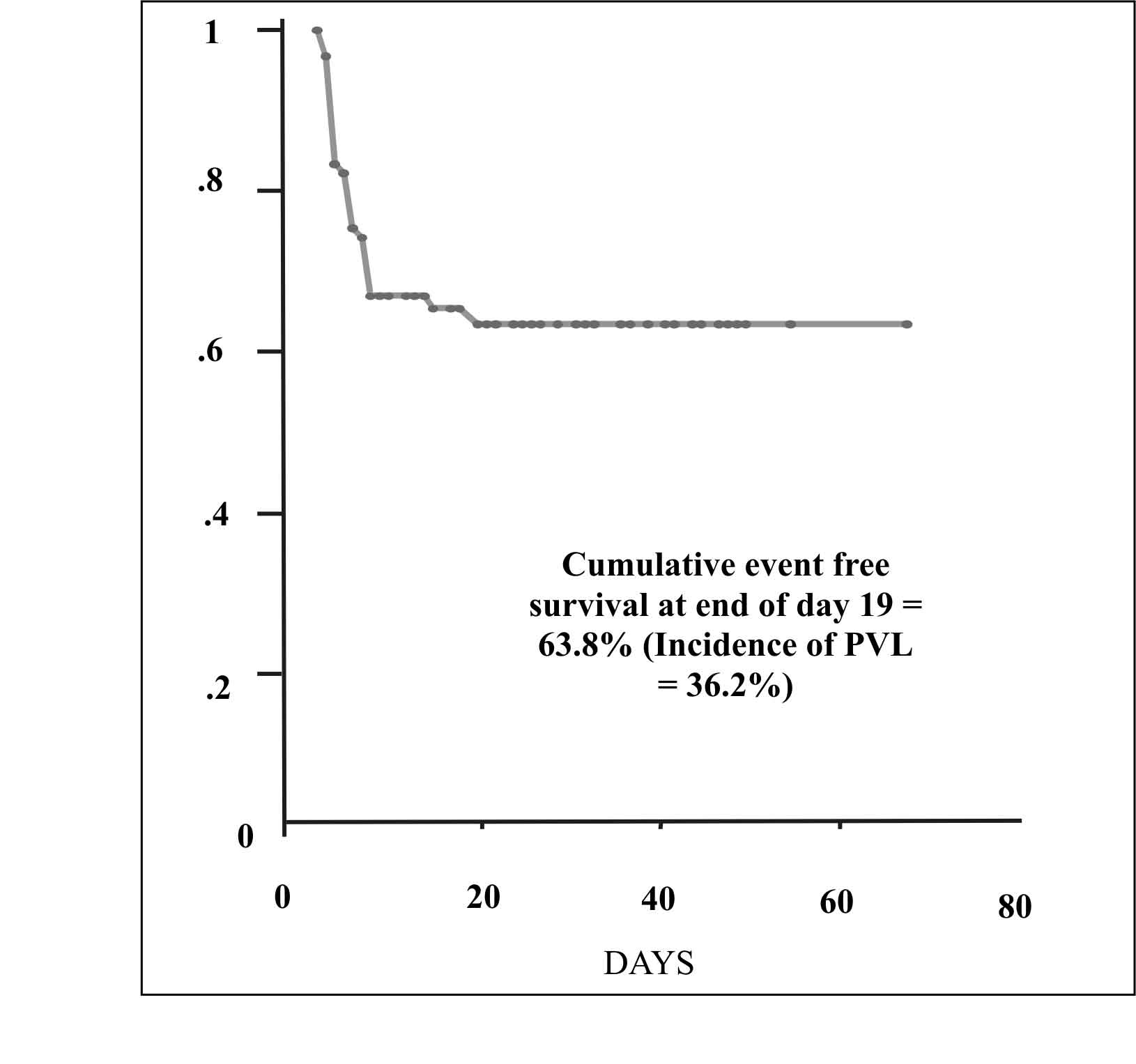
Periventricular leucomalacia (PVL) is a form of perinatally sustained brain damage involving periventricular white matter of the preterm brain. Until recently, intraventricular hemorrhage (IVH) was considered to be the most important form of preterm brain injury. In recent years, PVL is recognized as one of the most important predictor of adverse neuromotor outcome among high-risk preterm neonates(1). This should particularly be true as PVL is not a killer disease. Infact, PVL is more often seen among surviving VLBWs, rather than those dying in early neonatal period, who die perhaps before this disease process has evolved. However, data in this regard is merely speculative as no studies are yet available from India regarding issues such as incidence and natural history of peri-ventricular leucomalacia. Such knowledge about PVL in our set up would be an important prelude to getting any clues to strategies for prevention of PVL. Hence, the present study was conceived with objectives to diagnose, estimate incidence and describe natural history of PVL until discharge in a cohort of VLBW. Subjects and Methods A prospective cohort study was under-taken at a tertiary care hospital at New Delhi to include all inborn VLBW (<1500 g) neonates between April 2001 to May 2002. Small for gestational age (SGA) were defined as those with weight for gestation less than tenth centile on intrauterine growth charts(2). Neonates with major CNS malformation at birth or dying before first cranial ultrasound or getting transferred to another department within the first week of life were excluded. A verbal informed consent was taken, for serial cranial ultrasonographic examinations. An experienced pediatric sonologist performed serial weekly ultrasonographs (USGs) in both coronal and parasagittal planes, starting within 1st 7 days of life. The initial USG for a neonate who was sick and not fit enough to be transported, were performed in the nursery on an in-house Aloka Ultrasound scanner with 5 MHz transducer. However, once the baby was stable enough to be transported to radiology department, subsequent weekly scans were performed there, on HDI 3000 (ATL systems) scanner with a high resolution (4-7 MHz) electronic phased-array sector transducer with a small footprint. Ultrasound definitions and terminologies used: Serial ultrasound films of each subject were analyzed for presence of lesions compatible with diagnosis of PVL as per standard predefined criteria. Incident lesions were the lesions noted at the time of first detection. They could be either flares or cysts. An incident lesion of flare on ultrasound was defined as an area of increased echogenicity present in periventricular region, visible on both planes seen on two USGs at least 7 days apart such that the first USG should have been performed within 1st 7 days of life. Cystic PVL as an incident lesion on ultrasound was defined as echolucent lesions visible on both planes, in characteristic locations, present singly / multiple and not previously preceded by a flare. The incident lesions were followed up for documentation of natural history of PVL in form of Grade PVL (maximum grade of PVL achieved before discharge/death) and status of lesions before discharge or death. Evolution of lesions until discharge was described in terms of progression / regression/ persistence of ultrasound lesions. Progression for a flare was defined as either a unilateral flare turning into bilateral or breakdown of flare into cysts or even showing evidence of sequelae viz., cerebral atrophy / ventriculomegaly. Progression for cystic PVL was defined as either unilateral cystic lesion turning into bilateral or size / extent of cyst increasing. Any evidence of sequelae (cerebral atrophy/ventriculomegaly) in absence of grade III/IV. IVH was also taken as a form of progression. Regression for flare or cystic PVL was defined as complete resolution to apparent normalization without any evidence ever of progression. Persistence was considered when lesions remained unchanged before discharge. DeVries classification(3) of PVL grading on ultrasound was used: Grade I PVL is a prolonged periventricular flare present for 7 days or more. Grade II PVL is presence of small-localized fronto-parietal cysts. Grade III PVL is an extensive periventricular cystic lesion involving occipital and fronto-parietal white matter. Grade IV PVL consists of areas of extensive sub cortical cystic lesions. Statistical Methods Used Sample size ‘n’ was calculated for estimation of incidence and found to be to be 100 subjects using formula n = 4 pq/d2, assuming incidence of around 20% with permissible error of around 8% on either side at an alpha error of 0.05 and beta error of 0.2. Incidence and standard error with 95% confidence intervals for periventricular leucomalacia was calculated using Kaplan Meier (KM) survival analysis technique. Intra-observer reliability on ultrasound reporting was assessed using kappa statistics. Results There were 105 newborns eligible for the study during the study period. Eight babies were excluded; 1 requiring transfer to surgical unit and another seven died within first 3 days of life before first cranial ultrasound could be performed; so, the rest 97 VLBWs formed the prospective enrolled cohort. Base line characteristics Mean (SD) of birth weight and gestation in the cohort was 1173g (253 g) and 31.4 wk (2.8 wk) respectively. There were 47 males and 50 females. Almost 2/3 rd (64/97) were small for gestational (SGA) babies. Average (median) duration of NICU stay was 16 days (SD of 13d and range of 1-78 days). Average post conceptional age at discharge was 36±2weeks. Median number of ultrasounds per neonate was 4 (SD of 2.5 and range of 1-11). Overall deaths were 17 (17.5 %); 3 among PVL (about 10%) and 14 among non PVL group (about 21%). This difference was not statistically significant. Incidence of PVL Thirty-one babies out of the 97 babies developed PVL (including both forms of PVL i.e., flares and cysts). Last case of PVL was detected by 19 days of postnatal life. Using Kaplan Meier Survival analysis technique, the cumulative event-free survival at end of 19 days was 63.8% yielding an incidence of PVL as 36.2% (with SE of 5.3% and 95% CI as 25.8%- 46.6%). (Fig. 1).
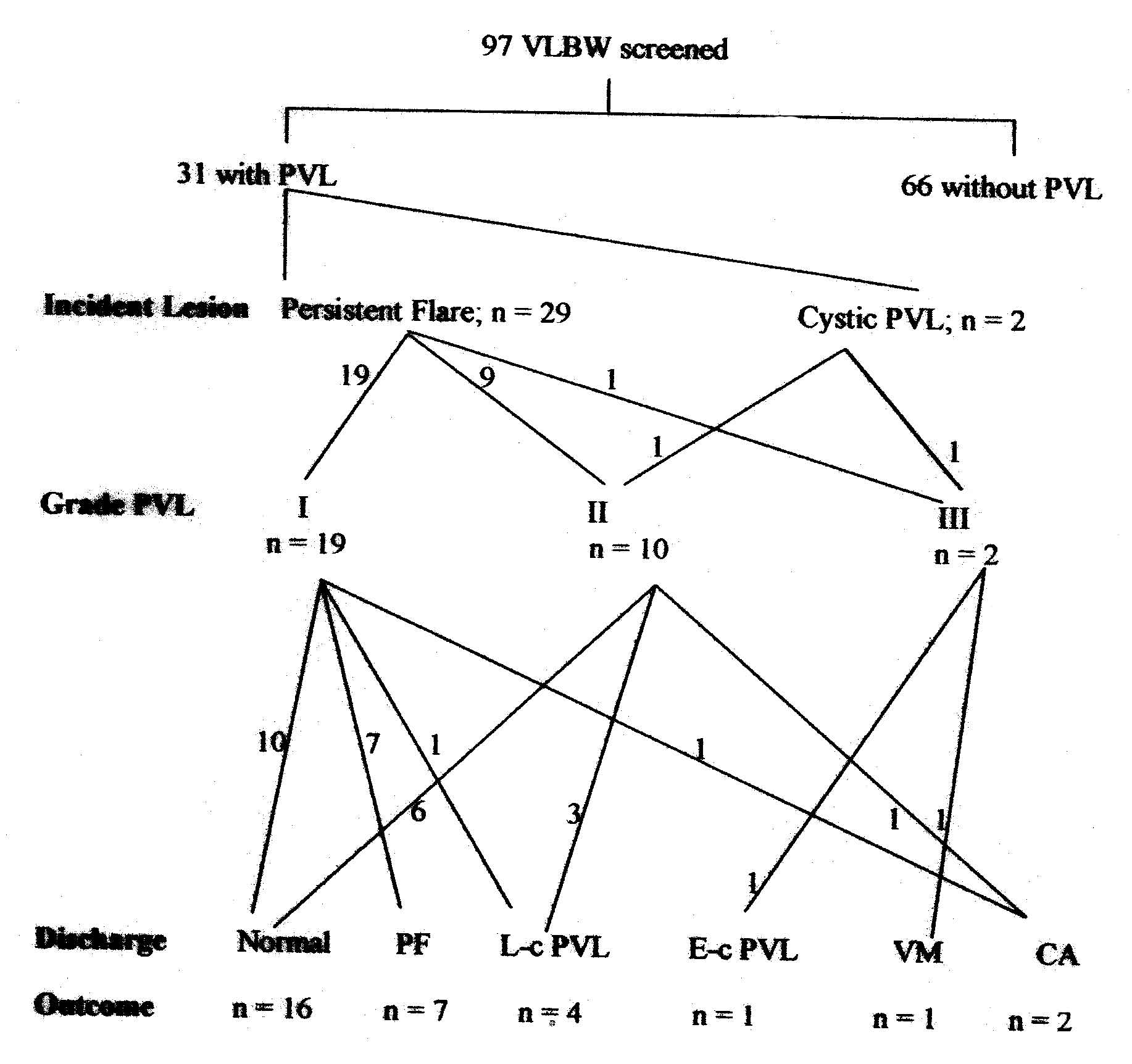
Natural history of periventricular leucomalacia Figure 2 shows distribution of three time strata of lesions in terms of incident lesions, Grade PVL and Ultrasound lesion status before discharge/death. The major incident lesion was a persistent flare seen in 93.5% cases (29/31) unilateral in 10 and bilateral in 19, while only 6.5% cases (2/31) had localized cystic PVL as the initial lesion.
When sonographic abnormality had progressed maximally to a level of persistent flare (Fig. 3 Grade I PVL), there was about 50% chance of the lesion to normalize before discharge, over 40% chance to persist and about 10% chance to either progress to cystic PVL or develop cerebral atrophy. On the other hand, if sonographic abnormality had progressed maximally to a level of localized cystic PVL (grade II PVL), they had 60% chances of normalizing, 30% chance to persist and about 10% chances to develop cerebral atrophy before discharge. The worst however, seemed to be cases which had progressed maximally up to extensive cystic PVL (Fig 4: grade III PVL), as none of them normalized; but had equal chances to either persist or develop sequelae of ventriculomegaly.
Intra-observer reliability on ultrasound reporting Criteria to diagnose PVL had been predefined. Intra-observer reliability was found to be more than 90% when same radiologist re-reported, the previously reported ultrasounds for each baby, being blinded to both i.e. to the clinical details as well as to his previous reporting of the same films. Where reporting differed, a final mutual consensus was reached in consultation with a second ultrasonologist. The diagnosis needed to be revised in only one case; from an initial label of ‘a large cyst of periventricular leucomalacia’ to a diagnosis of ‘porencephalic cyst’, as the echolucent area was preceded by an area of increased echogenicity suggestive of periventricular hemorrhagic infarction. Discussion Our incidence of 36.2% for all forms of PVL seems higher compared to that quoted from other studies(4-11). There exists a variability in incidence even among other studies reflecting the differences due to different inclusion criteria or variability in sonographic definitions used to describe the condition and possibly due to subjectivity inherent to the technique itself. All previous studies(4-11) have calculated incidence based on simple proportions. Fawer, et al.(7) found periventricular leucomalacia 29/120 infants <34 wks gestation. They used 7.5 MHz transducer, performed ultrasound daily during 1st week and then once weekly or more as required until discharge. DeVries, et al.(4) found an incidence of extensive cystic periventricular leucomalacia in 10/435 babies scanned. Recently Pierrat, et al.(9) in large study over 9 years from two hospital cohort reported an incidence of cystic PVL as 2.8% (96/3451) among preterm less than 32 weeks. None of the studies previously(4-13) has described an incidence based on survival analysis. We used this method to calculate the cumulative incidence rate. This takes care of the varying denominator with respect to time, as babies get discharged or die at varying interval of time before developing PVL. This kind of dynamic analysis is a moderate estimate, being neither extremely low, nor extremely high. Estimate would have been falsely low if only it was calculated using simple proportions as 31/97 (31.9%), which assumes all 97 subjects to be available for an equal length of follow-up. Estimate would have been falsely high if babies who died (n = 14) without developing PVL were excluded from the denominator. In the latter instance, an incidence of 37.4% (31/83) would be derived. However, survival analysis gives a more realistic figure of incidence estimate accounting for varying durations to discharge or death. Incidence lesions have been reported to be mostly flares by Rushton, et al.(5) and Trounce, et al.(6) like in our study. Incidence lesion as flares was found in 86% (17/24) at onset in a study by Fawer, et al.(7). In our study most lesions 93.5% (29/31) were noted as flares at onset. Unilateral flares Literature attests to the occurrence of these lesions as bilaterally symmetrica(l9,14-16). However, in present study we found one third of the flares were unilateral and two third were bilateral at the onset. Appleton, et al.(17) also has reported unilateral flares in 5/15 (1/3) cases. Localized cystic PVL The other type of incident lesion was found in 2/31(6.5%) cases as localized cystic PVL picked up to 19 days of postnatal life. Incident lesions as direct cysts were found in 14% (7/24) cases in Fawer’s(7) study, in 7.2% (7/96) cases in Pierrat’s(9) study. Outcome of lesion in relation to maximum grade of PVL achieved Applying same definition of persistent flares as used in our study, 4/7 (about 55%) of flares in study of Appleton, et al.(17) resolved before discharge and follow-up scans of other 3/7 cases were not available. In a recent study, Kreuzer, et al.(18) concluded that presence of a transient parenchymal echodensity i.e., a persistent flare of even 7 days’ duration was of clinical relevance as these ultrasonographic abnormalities have been associated with adverse neurodevelopmental outcome. Others have also reported similar findings in literature(19). Fawer, et al.(7) found most common sequence of PVL changes was an increased echogenicity, which progressed into cystic formation in 11/24 (about 45%) cases, persistent flares in 5/24 (20.8%) cases. Ventriculomegaly has been shown to be a marker of adverse neuromotor outcome(20). Pierrat, et al.(9) found cystic PVL in 2.8% cases. We found this in 2/97 (2%). However, subsequently during the natural history of progression there were overall 12 cases of grade II/III cystic PVL in our study. Out of these finally only four remained as cystic PVL (3 as localized cystic PVL and 1 as extensive cystic PVL), and one progressed to cerebral atrophy. There have been no studies describing epidemiology with respect to incidence, estimate and natural history of periventricular leucomalacia from India. Since our population consists of a large proportion of growth retarded babies with varied profile of maternal and neonatal high risk factor as compared to western population therefore we believe that we need to generate more data on incidence of PVL from our population in India. Contributors: AM, RA were responsible for initial drafting while AKD finalized the manuscript. AM ensured the follow up of enrolled babies. AG supervised the ultrasound examination. VS did the statistical analysis. VKP conceived the idea and AKD will act as guarantor of the study. Competing interests: None. Funding: None. .
| ||||||||||
|
References | ||||||||||
|
|
![]()