|
|
Original Articles Indian Pediatrics 2005; 42:223-231 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
†For this paper Dr. M. Upadhyay was awarded S.T. Achar Gold Medal of Indian Academy of Pediatrics at PEDICON-2001, Patna, Feb. 7-11,2001.
To compare the efficacy of crystalloid (Normal saline) and colloid (polymer from degraded Gelatin in saline- Haemaccel®) intravenous fluid in restoration of circulating volume in children with septic shock. Design: Prospective, randomized, open-label trial. Setting: Pediatric Emergency and Intensive Care Unit of a tertiary care referral and teaching hospital. Subjects and Inclusion Criteria: Sixty patients, between 1 month to 12 years of age, with septic shock, without clinical evidence of organ failure at admission or underlying immunodeficiency. Intervention: Resuscitation with normal saline or polymer from degraded gelatin (Haemaccel®) in the boluses rate of 20 mL/kg till hemodynamic stabilization or if central venous pressure (CVP) exceeded 10 mmHg (fluid requirement beyond 40 mL/kg guided by BP and CVP). Methods: Hemodynamic parameters (heart rate, capillary filling time, pulse volume, and blood pressure) were recorded before and during resuscitation, and then 2 hourly for12 hours. Central venous pressure line was placed within first hour, soon after starting fluids. Estimation of plasma volume and body water was done at the end of first hour of fluid resuscitation. Outcome measures: Hemodynamic stabilization (heart rate, capillary refill time, systolic BP in normal range), plasma volume at the end of fluid resuscitation and incidence of organ dysfunction. Results: 31 patients were randomized to normal saline and 29 to gelatin polymer. Both the groups were similar with respect to age, gender, primary diagnosis, initial hemodynamic parameters and PRISM score. Pneumonia (n = 22; 36%), gut-associated sepsis (n = 13), and dengue hemorrhagic fever (n = 11) were the common primary diagnosis. Initial hemodynamic stabilization was achieved in all. The mean ( SD plasma volume (saline- 53.4 ( 2.0 mL/kg, gelatin polymer- 53.2 (1.9 mL/kg), extracellular fluid volume, total body water and interstitial fluid volume at the end of first hour of resuscitation were similar. The requirement of inotropes, incidence of organ dysfunction and case fatality rate (Saline – 29%, gelatin polymer- 31%), were similar in two groups. Conclusion: Both normal saline and gelatin polymer solution were equally effective as resuscitation fluid with respect to restoration of plasma volume and hemodynamic stability. Normal saline upto 110 mL/kg, and gelatin polymer solution upto 70 mL/kg may be required in first hour for successful fluid resuscitation of septic shock in children. Septic shock is a form of distributive shock resulting initially from decreased vascular tone and capillary leakage leading to third space losses(1). Myocardial depression contributes to the shock in later stages(2,3). The mainstay of therapy in patients with septic shock is early and aggressive intra-venous fluid resuscitation and subsequent inotropic and/or vasopressor support(3). The speed and adequacy of fluid resuscitation is a major determinant of the final outcome as compared to an adequate antibiotic cover (4,5). However, the type of intravenous fluid that would be ideal for managing septic shock has been intensely debated(6-8). Arguments favoring use of crystalloids as well as colloids as fluid of choice for resuscitation in adult patients with septic shock have been presented. This study was designed to compare the efficacy of crystalloid (saline) and colloid (polymer from degraded Gelatin in saline) intravenous fluid in the emergency management of septic shock in children with respect to (i) restoration of plasma volume, (ii) improvement in hemodynamic status at the end of 6 hours and 12 hours of initial fluid resuscitation, (iii) the need for vasoactive drug therapy (number, maximal dose and duration) and (iv) survival. Subjects and Methods Design and sample size This was an open label randomized trial. Sixty patients admitted consecutively to pediatric emergency or ICU with a diagnosis of septic shock, between March 23,1999 to April 4, 2000 were enrolled in the study. They were randomized to receive either normal saline (Saline group) or polymer from degraded gelatin in saline (Haemaccel®, Gelatin group) for initial fluid resuscitation. Random numbers were generated with help of random number tables and were kept in sealed envelopes with one of the investigators (JM). No sample size estimation was done as main emphasis of the study was on quantitation of plasma volume. The study was approved by Ethics Committee of the Institute. An informed written consent was obtained from parents. Inclusion Criteria Patients 1 month - 12 years with septic shock were included in the study. Septic shock was defined as sepsis and hypotension (systolic BP <70 mmHg in infant ; <70 +2 × age after one year of age) OR sepsis with three of the following four clinical signs of hypoperfusion: decreased pulse volume, capillary filling time ≤3 sec, tachycardia (heart rate >190/min in 1 month to 2 year, >140 /min in 2 to 8 years and >110/min in >8 years) and urine output <1 mL/kg/hr (<20 mL/hr in >20 kg child).Exclusion Criteria Patients presenting with features of multiorgan failure such as disseminated intravascular coagulation (DIC) with bleeding manifestation, jaundice, acute renal failure, adult respiratory distress syndrome, coma, age less than one month and underlying immunodeficiency states such as leukemia, lymphoma, long-term immunosuppressive therapy were excluded. Fluid Protocol Once a clinical diagnosis of septic shock was made and the eligibility criteria satisfied, the child was randomized to fluid resuscitation with polymer from degraded gelatin (Haemaccel®) or normal saline. Continuous monitoring of heart rate, respiratory rate, and blood pressure was started. Central venous lines was established within the first hour of resuscitation and fluid resuscitation with the same fluid was continued in boluses of 20 mL/kg every 10-20 minutes till blood pressure returned to normal, perfusion improved or central venous pressure was >10 cm H2O. Episode(s) of hypotension, if any, after initial stabilization were also treated with the same fluid. Inotrope(s) / vasopressors(s) were given if hypotension or poor perfusion persisted and the CVP was >10 cm H2O. Dopamine was the first choice; epinephrine was considered if dopamine (at rate of 20 micro-gram/kg/min) failed to stabilize the blood pressure. Dobutamine was used if there was poor peripheral perfusion with no hypotension, Measurement of plasma volume body water Two mL/kg of a solution containing Evans blue (0.4 g/L), tritiated water (3 µCi) and sucrose (0.6 mmol/mL) was injected intravenously at the end of resuscitation and blood samples were collected before injection and at 20, 40, 60,120 and 180 minutes of injecting the dye. Plasma volume was estimated by measuring dilution of Evan’s Blue in plasma samples obtained at 0, 20, 40 and 60 minutes(9). Extra-cellular water (ECW) and total body water (TBW) estimations were done on plasma samples obtained at 0, 60, 120 and 180 minutes by measuring sucrose space by method of Zweens and Frankena(10), and by counting volume of distribution of 3H activity in plasma water(11) respectively. Interstitial water compartment was calculated by subtracting plasma volume from ECW, and intracellular water was calculated by subtracting ECW from TBW. Monitoring Heart rate, respiratory rate, capillary filling time, pulse volume, and blood pressure were recorded before starting the fluid resuscitation, during the fluid resuscitation, at the end of one hour, and thereafter every 2 hours. The Pediatric Risk of Mortality (PRISM) score was assigned at 12 hours post-admission(12). Blood samples for serum sodium, potassium, blood urea, creatinine, blood gases, hemogram with platelet counts and bacterial culture were taken before starting therapy with antibiotics (selection of which depended on patient’s age, focus of infection and likely organisms and their known susceptibility pattern). Culture of urine, stool, pus, cerebrospinal fluid and any other body fluids were also obtained depending on the suspected location of sepsis. Complete blood count, coagulation parameters and renal function test were monitored every 12-24 hours and arterial blood gas every 6 hours. The intensive clinical monitoring was continued until patients became hemodynamically stable for at least 6 hours after that it was continued at increased interval until patients recovered. Hemodynamic Stability was defined as BP above 5th percentile, with pulse rate within normal range for age, urine output >1 mL/kg, and capillary refill time <3 sec (any two). Central venous pressure was considered as normal if it was between 6-8 cm in infants and 8-12 cm H2O beyond infancy. Standard definitions were used for sepsis and organ dysfunction as shown in Table I(13). Table I Definitions Used in the Study (adapted from reference 13).
Statistical Analysis Descriptive statistics (mean and standard deviation or median and interquartile range/weighted percentile) were calculated. Between groups comparison of continuous variables was done with help of t-test for parametric data and by Mann-Whitney U test for non-parametric and ordinal data. The proportion and frequencies were compared by using by Chi-square test (with Yates correction) or Fisher’s exact test. Results Of the 60 patients 35 were under 5 years of age, and 45 (75%) were boys. Fifty-three patients either had a focus of infection or a clearly identifiable systemic infection. The most common infection was pneumonia (36%). A bacterial organism could be identified in 9 (15%) and 7 (12%) were seropositive for dengue. Both the groups were matched with respect to the age and sex distribution and were similar with respect to the basic diagnosis, blood culture positivity, positive serology, initial hemodynamic parameters and PRISM score (Table II). Table II General Characteristics and Hemodynamic Variables at Admission.
Values mentioned are a median (Inter
Quartile Range), b number of children (percent), c mean ± SD. At the end of fluid resuscitation Saline group and Gelatin group had similar plasma volume, total body water, extracellular fluid volume, interstitial fluid volume, plasma osmolality and urinary osmolality (P >0.1, Table III). Intracellular fluid volume was lower in the saline group compared to the colloid group (P <0.05). TABLE III Plasma Volume, Body Water and Clinical Outcome.
aAll values are Median ± IQR,
bthe denominator has changed because some patients died by this
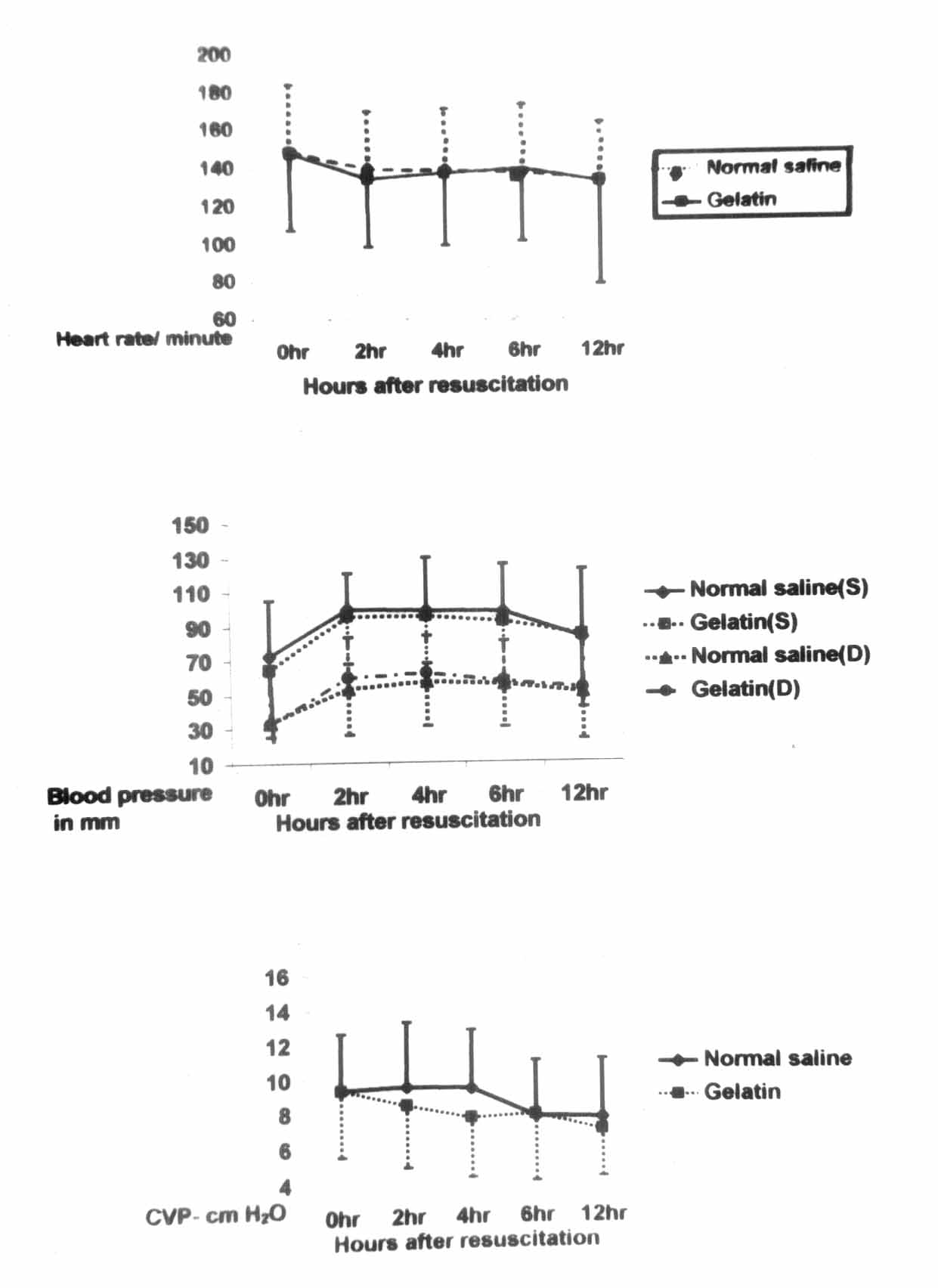
time. Median (10th-90th percentile) volume of fluid needed for initial resuscitation was 50 (20-108) mL/kg in Saline group and 30 (20-70) mL in Gelatin group. (P = 0.018, Mann Whitney U). The median (10th-90th centile) time taken for fluid resuscitation was 45 (15-98) minutes in saline group and 35 (15-90) minutes in Gelatin group (P = 0.41, Mann- Whitney U). Both the groups were similar with respect to the hemodynamic stability at 6 and 12 hours of admission (Table III). The overall trend of hemodynamic parameters in both the groups was similar (Fig. 1).
The overall requirement of vasoactive drug infusion was similar in both the groups; no vasoactive drug was required in 12 and 8, one drug in 9 and 16, and two or more were needed in 10 and 5 patients from Saline and Gelatin group respectively (P >0.05). The median (inter-quartile range (IQR) duration was 18 (9.4-30.1) hours among 19 patients in Saline group, and 18.5 (7.6-73.8) hours in 21 patients in Gelatin group who needed vasoactive drugs (P >0.05). The survival rate and incidence of organ failure was similar in both the groups (Table III). The PRISM scores (median, 10th-90th centile) of non-survivors(12,8-18) were significantly higher than the survivors(6,3-8) (Z-score-3.8, P < 0.0001, Mann-Whitney U). Discussion Both the fluids, saline and gelatin polymer in saline, titrated on the basis of clinical hemodynamic end-points and CVP were able to achieve similar expansion of plasma volume. There was no statistically significant difference between the plasma volume, extra cellular water and total body water in both the fluid groups at the end of resuscitation. Our findings provide rational for survival benefits observed with timely rapid resuscitation, directed at rapid restoration of hemodynamic parameters irrespective of fluid used, whether crystalloid or colloid(14,15). Experimental studies in animal models of septic shock have generally favored the view that colloids are more effective in restoration and maintenance of circulating volume, mostly because of their oncotic effect. Marx, et al.(16) studied effect of four different fluids (Gelatin 4 and 8%, 6% hexaethyl starch, and Ringer’s solution) to maintain a CVP at 12 mm Hg on plasma volume in a porcine model of septic shock. Colloid resuscitated groups successfully maintained their plasma volume. In contrast, animals on Ringer’s lactate showed a significant decrease in plasma volume and intrathoracic blood volume, and increased hemoconcentration(16). Apparently, these well controlled experimental circumstances do not apply to clinical scenario of septic shock in human subjects. The median volume of fluid required for resuscitation with saline was 20 mL/kg more than that needed with gelatin polymer. This is consistent with findings that for achieving similar hemodynamic end-points and a target pulmonary arterial wedge pressure, significantly larger amount of saline is required(17). However, Choi, et al.(8) in their meta-analysis found that fluid required for resuscitation in crystalloid and colloid group was not statistically different. The hemodynamic trend in both the study groups was similar, though CVP remained somewhat higher in first 12 hours in normal saline group. Both the groups required fluid boluses after 6 hours up to 24 hours to maintain hemodynamic stability. Our data suggest that the factor of capillary permeability affects both the fluids in a nearly similar manner. This is in contrast to data in adults. Haupt, et al.(18) found that to maintain adequate pulmonary capillary wedge pressure in first 24 hours following initial fluid resuscitation, patients in crystalloid group required more fluid boluses than those in colloid group. Rachow, et al.(17) observed that to maintain hemodynamic stability the total fluid requirement in saline group during maintenance phase was 2 to 4 times more than albumin or hetastarch. The requirement of vasoactive drugs was similar in the saline and gelatin treated group. This was similar to that found by the study of Carcillo, et al.(3) where the mean number of inotropic drugs required was 1.5 at 6th hour of resuscitation. A higher incidence of pulmonary edema has been reported in patients receiving saline, which was attributed to a fall in colloid osmotic pressure(17). We did not see pulmonary edema following fluid therapy in either group, though one patient in gelatin group developed ARDS on second day of hospital stay. Our finding is in accordance with finding of the meta-analysis by Choi, et al.(8) that there is no difference in incidence of pulmonary edema in recipients of crystalloids or colloids(8). The survival rates and incidence of organ failure was similar in the Saline and Gelatin groups. Although, the study was not powered to study the survival benefits, our findings go well with the recently published data(5) and should contribute to resolution of crystalloid versus colloid controversy. Two meta-analyses reported marginal benefit if any with crystalloids or colloids; one reported higher risk of death with crystalloids(7) other found a 4% increased risk with colloids. The overall high mortality in both the study groups was probably due to late presentation of the most of the patients to the referral hospital and severity of illness. The patients who died in either group had a much higher initial PRISM score than those who survived. Choi, et al.(8) postulated that factors such as acute illness severity, co-morbidity and ICU acquired complications have more powerful influence on mortality of shock than the type of fluid used for resuscitation. In conclusion, our data support that both the saline and gelatin polymer were equally effective resuscitation fluids for septic shock in children with respect to restoration of plasma volume and hemodynamic stability, and maintenance of hemodynamic stability over next 24 hours. The data support use of normal saline upto about 110 mL/kg within first hour for initial resuscitation of patients with septic shock. Saline may be prefered to gelatin polymer solution in view of its comparable efficacy, low cost and ready availability. Acknowledgement The authors thank Drs. J.A. Carcillo and G. Venkatraman for critical review of manuscripts and helpful suggestions. Contributors: MU: preparation of the protocol, clinical data collection, draft of the manuscript; SS: conceptualisation of research, critical appraisal of protocol, final manuscript; JM: supervision and monitoring of data collection; SM: supervision and monitoring of Laboratory work; and NK: estimation of body water-laboratory work. Funding: None. Competing interest: Nil.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()