|
|
Case Reports Indian Pediatrics 2003; 40:258-260 |
|||
|
An Unusual Case of Neonatal Anuria |
|||
|
N. Prasad From the Departments of Nephrology, Pathology and Anesthesiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226 014, India. Correspondence to: Dr. Sanjeev Gulati, Department of Nephrology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareli Road, Lucknow 226 014, India. Manuscript received: September 9, 2001; Initial
review completed: October 9, 2001;
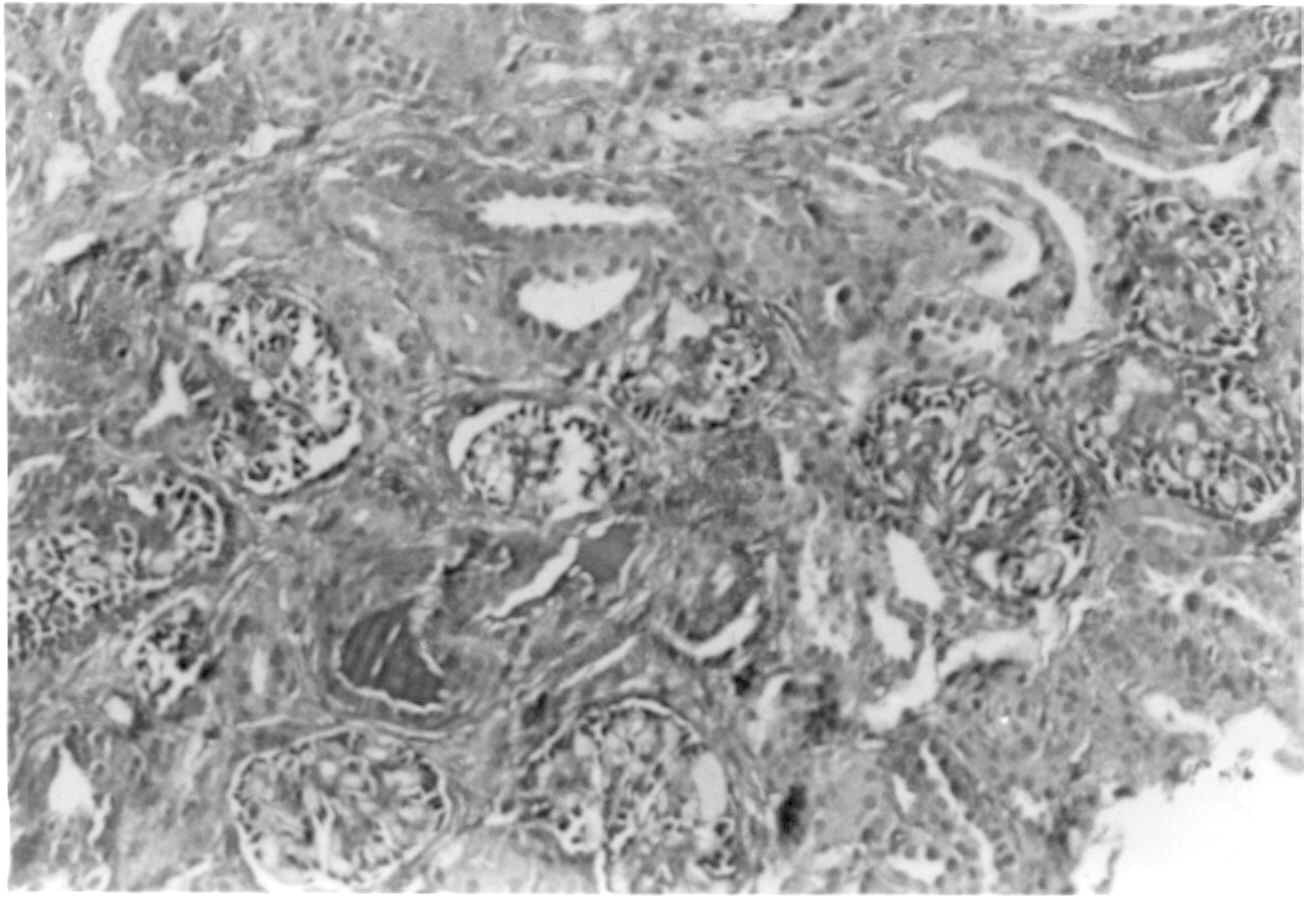
Neonatal anuria is not an uncommon problem seen in neonates. It is defined as failure to pass urine for 24 hours after birth. Acute renal failure in newborn occurs in about 8% of admissions in neonatal intensive care unit(1-7). Neonatal acute renal failure can be due to prerenal, renal and post-renal etiologies. Intrinsic renal causes accounts for about 6% cases of neonatal acute renal failure. Here, we report an unusual case of neonatal anuria due to renal tubular dysgenesis, secondary to the use of an angio-tensin converting enzyme (ACE) inhibitor during pregnancy. Case Report A 26-year-old gravida 4 mother delivered a boy at 33 weeks gestation. The child was referred for not having passed urine for 48 hours after delivery. The urinary bladder was empty on catheterization. Previous obstetric history revealed that the first two female children were normal. The mother had pregnancy induced hypertension during the third pregnancy and was prescribed enalapril at dose of 5 mg 12 hourly during the second and third trimester. That pregnancy ended in a still birth at 32 weeks gestation. During this pregnancy, she again continued to take enalapril upto the third trimester. An antenatal ultrasound at 27 weeks showed oligohydramnios. Treatment with enalapril was inadvertently continued. She delivered a 2.1 kg boy at 33 weeks gestation. There was no birth asphyxia. General physical examination showed pulse rate of 110/min and blood pressure 80/50 mm Hg. The neonate also had hypocalvaria and bilateral talipes equino- varus. Rest of systemic examination was unremarkable. Postnatal ultrasound showed right kidney of 48 mm and left kidney 53 mm, which were normal for age. There was no evidence of hydronephrosis and the urinary bladder was normal. Investigations showed hemoglobin level of 13.8 g/dL, total leucocyte count 9,600/cumm, blood urea nitrogen 37 mg/dL, creatinine 2.4 mg/dL and potassium 4.5 mEq/L. The peak serum creatinine and potassium levels were 7.5 mg/dL and 5.6 mEq/L respectively. As the child continued to be anuric, a cuffed Tenckhoff catheter was inserted under general anesthesia and he was commenced on peritoneal dialysis. An ultrasound guided kidney biopsy on the sixth day of life showed 28 glomeruli, which showed prominent visceral epithelial cells, tubular focal dilation and absent differentiation of proximal convoluted tubules. These findings were suggestive of renal tubular dysgenesis (Fig. 1). The neonate passed urine on the eighth day of life. Urine microscopy was normal. The child received intermittent peritoneal dialysis via the Pac-Xtra PD cycler. Blood chemistry on the eighth day of life showed a blood urea nitrogen of 40 mg/dL and creatinine level of 4 mg/dL.
In view of anuria after birth, history of enalapril intake by the mother during pregnancy, oligohydramnios, renal tubular dysgenesis, hypocalvaria and bilateral talipes equinovarus, a diagnosis of ACE inhibitor induced neonatal anuria was made. Due to financial constraints and poor long term outcome, the parents opted to discontinue peritoneal dialysis after 18 days and the boy was discharged on request. Discussion ACE inhibitors have emerged as the first line antihypertensive of choice due to their renal modulating effect. Studies have shown that there is a risk associated with the use of ACE inhibitors during the second and third trimesters of pregnancy. Enalapril can cross the placenta in developing fetus(2). Excretion of ACE inhibitors is principally through the kidney. In the fetus, it is presumed that ACE inhibitors are renally excreted into amniotic fluid and recycled by fetal swallowing(8). These drugs are believed to have pharmaco-logical effect during fetal period of development, stage of pregnancy from eighth week after conception till term. Recently, there are case report of adverse effect of its use in the first trimester and use of these drugs should be avoided in all trimesters of pregnancy(9). In the present case, there was history of previous still birth at 32 weeks’ gestation. The present patient had oligohydramnios, anuria, hypocalvaria and renal tubular dysgenesis similar to other case reports of ACE inhibitor induced fetopathy(1-5). Membranous bones require a high degree of vascularity and high oxygen tension during fetal development. ACE inhibitors cause profound hypotension and hypoxia thus resulting in hypoplastic calvaria(7). Transfer of ACE inhibitor across the palcenta may decrease angiotensin II level in the fetus. This would have the dual effects of decreasing systemic blood pressure and the compensatory efferent arteriolar tone. This would result in low glomerular filtration pressure, reduced urine production, oligo-hydramnios and neonatal anuria(8). We conclude that ACE inhibitor induced renal tubular dysgenesis is an unusual but important cause of neonatal anuria. ACE inhibitors are one of the most commonly used antihypertensive drugs inadvertently prescribed to women during pregnancy. Following ACE inhibitor therapy, it is estimated that 50% infants may be affected and 25% die(8). ACE inhibitors should not be prescribed during any trimester of pregnancy. A greater awareness needs to be created in the medical faternity especially among pediatricians, gynecologists and internists. Contributors: NP was involved in data collection and drafting the manuscript. SG was involved in clinical management and critical review of the manuscript. MJ reported the kidney biopsy and helped in data collection. PT provided anesthetic back up during biopsy, catheter insertion and drafting of the manuscript. Funding: None. Competing interests: None stated.
|
![]()