|
|
Case Reports Indian Pediatrics 2002; 39:292-295 |
||
|
Benign Familial Neonatal Convulsions |
||
|
Jatinder S. Goraya Verinderjit S. Virdi Veena R. Parmar
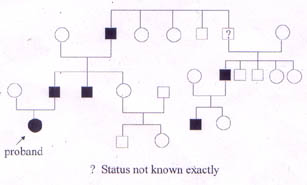
Neonatal seizures usually indicate a significant underlying neurological disorder. Although etiology of neonatal seizures is multiple and diverse, only a few of these conditions account for most seizures. Very few seizures during the newborn period are idiopathic. The prognosis is variable, determined primarily by the underlying etiology(1). Benign familial neonatal convulsions (BFNC) represent a distinctive epileptic syndrome of neonatal onset and a favorable prognosis(2). The syndrome is characterized by the occurrence of unprovoked partial or generalized clonic seizures in the neonatal period or early infancy. There are no pre-or perinatal adverse antecedents and findings on neuroradiological and biochemical examina-tions are normal. Brief seizures occur for several days or weeks and then regress spontaneously. There is a positive family history with an autosomal dominant inheritance pattern for neonatal seizures. Affected individuals show normal psycho-motor development(3,4). Recognition of this syndrome is important for it not only allows the prediction of a favorable prognosis from the neonatal period but also helps in avoiding unnecessary investigations and therapeutic interventions. We describe a family with BFNC, probably the first such family to be described from India. Also importance of family history in investigation of a neonate with seizures is highlighted, because the diagnosis of BFNC in this infant was made in retrospect at about one year of age, when historical information was reviewed. Case Report The proband, currently 2-year-old girl, product of non-consanguineous parents was born at term by normal vaginal delivery after an uneventful gestation. At 2.5 months of age she presented with convulsions. The ictal event consisted of deviation of eyes to right side with clonic jerks involving right side of the body including face, arm and the leg. Each episode lasted 2-3 minutes and about 25-30 episodes occurred during the ensuing week. These episodes occurred during awake hours or shortly after awakening, but never during sleep. Examination revealed no neuro-cutaneous markers and normal neurological status. Investigations revealed normal hemogram, blood sugar of 102 mg/dl, serum calcium of 9.6 mg/dl, and serum magnesium of 1.8 mmol/L. Computed tomography (CT) of head was normal. Electroencephalography did not reveal any abnormality. The infant was initiated on oral phenytoin. She remained well till about 15 weeks of age when she had recurrence with 4 episodes of short lasting seizures. Subsequently she did not experience similar or any other type of seizure. At 17 months of age when she was seen by one of the authors (JSG), very strong family history of seizures up to three generations was noted (Fig. 1). The affected family members had similar types of seizures during the early life (the onset reportedly ranged 3 days to 2 months of life) and the seizures appeared in clusters lasting a few days. None received long-term anticonvulsant medication. No other kind of seizures occurred and epilepsy or psychomotor dysfunction did not result in any of them. However, no medical records are available for scrutiny. Following this the diagnosis of benign familial neonatal convul-sions was made and anticonvulsant therapy tapered off successfully without any seizure recurrence. The child has shown normal neurodevelopment. Discussion Benign familial neonatal convulsions are recognized as a distinct epileptic syndrome of neonatal onset, favorable outcome and familial occurrence(2). It is a rare disorder, and is probably under-recognized(3). Rett and Teubel(5) reported the first family with BFNC in 1964 and the first case report in the English literature appeared in 1968(6). The disorder has been reported in more than 45 families so far, with none from India(3). Benign familial neonatal convulsions have a characteristic presentation. Seizures occur in previously healthy full-term neonates born after a normal pregnancy and delivery(3). The sex distribution is equal. In majority of cases seizures start on the second or third day of life (6-11), onset as late as the third month(8) has been reported. Our patient had seizures at 2.5 months of age, which is well within the reported range. The interictal period is unremarkable. The ictal episode, which has been better characterized after the introduction of video-EEG monitoring(7,9), consists of a tonic phase, followed by various autonomic and motor changes. Seizures in BFNC frequently are genralized tonic clonic, but focal or multifocal clonic convulsions have also been reported. Seizures are short lasting (1-3 minutes) and are frequently repeated within a period of 1-7 days. Other types of seizures do not occur(3). Some of the seizures in our patient occurred on arousal, an observation that has previously been well documented(7,9).
Fig. 1. Family pedigree Occurrence of seizures in the proband and her family members showed autosomal domi-nant inheritance, consistent with BFNC(3). Genetic heterogeneity, however, is known as the genetic loci have been found on chromosomes 20q(12) and 8q(13). A family without these genetic loci also has been reported(14). Recently, potassium channel gene mutations have been found to be the underlying cause for BFNC(15). We did not have access to these molecular studies. The diagnosis of BFNC is based on a family history, and exclusion of other causes of neonatal seizures. Since the diagnosis of BFNC cannot be made in the absence of family history, meticulous attention should be paid to this aspect to prevent the oversight of the diagnosis as happened in our case. Though there can be recall problems, the age of onset as well as the remission of seizures in the family members conformed to that of BFNC. Laboratory evaluation, such as serum electolytes, glucose,calcium, and magnesium, are within normal range(3). The EEG is of limited value. Interictally it may be normal discontinous, or shows focal or multifocal abnormalities including so called theta pointu alternant pattern(7). Ictal EEG consists of generalized flattening of the background activity, followed by localized or generalized spikes or slow waves(8). Neuro-imaging is usually not indicated(3,11). The benign familial neonatal convulsions must be differentiated from non-epileptic paroxysmal phenomenon like benign neonatal sleep myoclonus (BNSM) and from other types of neonatal seizures. Myoclonic jerks in BNSM appear only during sleep, stopping immediately on awakening(16). Symptomatic neonatal seizures usually secondary to hypoxic-ischemic encephalopathy, metabolic disturbances, or infectious processes differ from BFNC in regard to onset, clinical type of seizures, duration and repetition of seizures, neurological state, and EEG patterns(1,3). Seizures in benign idiopathic neonatal convulsions are rarely familial, occur during a narrow age window, starting on days 4 to 5, and lasting no more than few days, and are never tonic(3). Seizures in benign infantile familial convulsions are partial and like BFNC, occur in previously neurologically normal infants, appear in a cluster, and are brief. Family history suggests autosomal dominant transmission. However, seizure onset is beyond 3 months, commonly between 4 to 7 months(17). Treatment of BFNC is not clear because many seizures remit spontaneously(3). Conventional anticonvulsants have been tried, many times without any benefit(4,6,11). If treatment is initiated at the time of seizures it is advisable to interrupt it by the third or sixth month(3). Long-term prognosis of BFNC is excellent. The seizures remit in majority of them by 6 months of age. Psychomotor development remains normal. Risk of subse-quent epilepsy is increased and has been estimated to be between 13 to 20%(4,8,10). The increased risk is associated with some but not all pedigrees suggesting hetero-geneity(4,11). Unexpected deaths have been reported(6). In conclusion, BFNC should always be considered in the differential diagnoses of neonatal seizures. Elicitation of family history will clinch the diagnosis and help avoid un-necessary investigation and prolonged treat-ment with potentially toxic agents. Moreover, it will allow early prediction of prognosis. Contributors: JSG, VSV were involved in literature search and preparation of the manuscript. VRP co-drafted and critically evaluated the paper. JSG will act as the guarantor of the paper. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()