|
|
Case Reports Indian Pediatrics 2002; 39:288-291 |
||
|
Stridor in an Infant – A Rare Cause |
||
|
Banani Poddar* Nitin Nagarkar Durlabh Shah Bishnoi* Arjun Dass
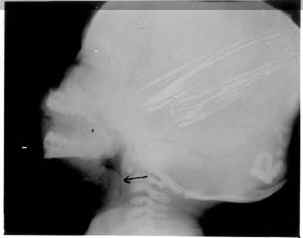
Stridor in early infancy is caused by congenital anomalies of the airway in a large majority of cases, laryngeal anomalies being most common(1). Congenital laryngeal cyst, especially of the saccular type, is a rare developmental anomaly which presents with stridor since infancy and is eminently treatable(2). We present a case of congenital saccular cyst of the larynx who had stridor and failure to thrive and was successfully managed. Case Reports A 4 month-old male baby was admitted to the pediatric emergency with a history of noisy and labored breathing since the neonatal period. He was a term home delivered baby of average birth weight and had no asphyxia. Parents noticed noisy and labored breathing unrealated to posture since the 3rd day of life. There was no apparent difficulty in breast-feeding, though, they noticed that he was not growing well. A history of drooling of saliva off and on was obtained on direct questioning. Examination revealed a wasted baby weigh-ing 2.5 kg with tachypnea (respiratory rate 64/min), suprasternal recessions and inspiratory stridor. There were no obvious congenital malformations or dysmorphism. The rest of the systemic examination was unremark- able. Bed-side direct laryngoscopy showed a smooth cystic swelling obscuring the laryngeal inlet. Lateral radiograph of the neck showed a radiolucent well-defined smooth swelling compromising the upper airway, arising from the supraglottis (Fig. 1). Ultrasound of the neck confirmed the cystic nature of the lesion (size 1.3 × 1.5 cm). Direct laryngoscopy using a rigid laryngoscope was done under general anesthesia after securing the airway (tracheostomy). A smooth walled cyst was seen arising from the left arye-pigiottic fold. Deroofing of the cyst was done. Histopathological examination demonstrated the cyst lined with squamous epithelium with a few lymphomononuclear cells consistent with laryngeal cyst (saccular type). The postoperative period was uneventful and he was decannulated on the 7th postoperative day after repeat direct laryngoscopy. He was discharged on the 11th postoperative day. He has been on regular follow up and after six months, there is no recurrence of the cyst and he has gained 8 kg weight.
Fig. 1. X-ray soft tissue lateral neck of the patient showing a radiolucent smooth-walled swelling arising from the supraglottis. Discussion Stridor is the audible symptom produced by the rapid, turbulent flow of air through a narrowed segment of the large airways(3). Inspiratory stridor typically originates from a glottic or supraglottic obstruction while expiratory and biphasic stridor denote sub-glottic obstruction. It is the most prominent symptom of airway obstruction in the pediatric patient(3). Congenital laryngeal cyst is a rare cause of airway obstruction which presents in the neonatal period or early infancy; the largest single centre series collected only 20 cases over a 15 year period(4) and Indian studies are scarce(5,6). Delay in diagnosis and treatment may lead to serious morbidity and mortality and hence their importance. Laryngeal cysts are classified as ductal or saccular types(7). Saccular cysts arise in the saccule of the ventricle and hence are more likely to cause early airway compromise. Ductal cysts, on the other hand, are mostly situated in the vallecula and usually cause feeding problems before obstructing the airway(8). Failure to thrive has not been described frequently with saccular laryngeal cysts but was present in our patient(2). Due to the difficulty in swallowing, the baby was probably taking small volume feeds and hence had failure to thrive. The other modes of presentation include an abnormal cry, coughing and episodes of cyanosis(2). The diagnosis is suggested by a lateral neck radiograph and can safely be confirmed by fiberoptic (transnasal) laryngoscopy(2,8). CT and MRI are helpful in delineating the location and extent of the lesion(3). Direct laryngoscopy, however, is regarded as a gold standard(5). Management includes: (i) securing the airway immediately, especially in patients with severe respiratory obstruction, and (ii) removal of the cyst. A choice between endo-scopic removal (where the cyst can be marsupialized, excised or de-roofed) and external approach (in the form of laryngo-fissure or lateral cervical approach) exists. Endoscopic removal is regarded as the treatment of choice, with external approach reserved for recurrence(8,9). Carbon-di-oxide laser can also be used as a modality of treat-ment for excision of the cyst(2). Endoscopic deroofing is technically simple and has an effective cure without recurrence(8). In conclusion, congenital saccular laryn-geal cyst is a rare cause of airway obstruction leading to stridor, presenting in early infancy. Failure to thrive can also occur as in our patient. Direct laryngoscopy under general anesthesia confirms the diagnosis and endo-scopic deroofing is a simple and effective therapy. Contributors: BP and NN conceived the idea and drafted the paper. DSB and NN managed the patient and helped in drafting the paper. AD edited the manuscript. BP will act as the guarantor for the paper. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()