With the
advancement in the field of technology, the use of educational
technology tools in medical education are on the rise. The 2007,
Effective use of educational technology in medical education
report of the Association of american medical colleges institute
for improving medical education (AAMC-IME) highlighted the
effectiveness of educational technology in medical education and
emphasized that for designing instructional presentations for
medical students, medical educators must apply the principles of
educational technology learning [1]. Broadly, medical
educational technology can be divided in to three functional
divisions – computer-aided instructions (CAIs), virtual patients
(VP), and human patient simulation (HPS).
Of the three functional divisions of
medical educational technologies, CAIs in the form of use of
multimedia is the most frequently utilized aspect in medical
education. Sensing the utility of medical educational
technologies and multimedia, many regulatory bodies started
faculty development programs, focusing on this aspect. The
Medical council of India (MCI) Basic course workshop in medical
educational technologies (BCW-MET) covers the area as ‘Improving
self-directed learning through technology’ [2]. From 2015, MCI
has made it mandatory for medical colleges to make adequate
provisions for conversion of lecture theatres in to E-class and
virtual class rooms [3]. As per the competency-based
undergraduate medical curriculum, establishment of skill labs by
December, 2019, in order to enhance students’ clinical, motor,
communication skills and team work in medical colleges, has also
been made mandatory by MCI, and guidelines for the same were
issued recently [4].
The premise that medical students
learn better with the use of multimedia and CAIs is based on
sound theoretical rationale and empirical evidence, some of
which is discussed herein.
Theoretical Rationale: Theory of
Multimedia Learning
People learn better from a combination of words and pictures,
than words alone. This multimedia principle makes the basis of
theoretical rationale of multimedia learning [5]. Accordingly,
Mayer gave a cognitive theory of multimedia learning, stating
that meaningful learning using multimedia is more likely to
happen if multimedia instructional messages are designed keeping
in view how the human mind works [5]. The theory is primarily
based upon four scientific criteria – theoretical plausibility,
testability, empirical plausibility, and applicability. This
theory is based upon three fundamental assumptions [5] (Box
I).
Box I Three Fundamental
Assumptions of Cognitive Theory of Multimedia Learning
• Dual channels: Human information processing system
has separate auditory / verbal channels and visual /
pictorial channels, which then work together to make
cross-channel representations.
• Limited
capacity: Humans have limited capacity of processing the
information through each channel, at a time, the
assumption being consistent with the cognitive load
theory
• Active processing: In humans active
learning happens by constructing a coherent mental
representation of experiences, and by integrating
incoming information with the prior knowledge – making
mental model. |
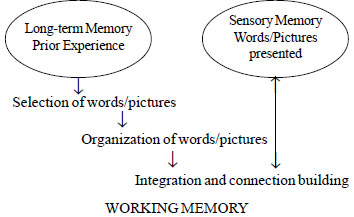
As per the cognitive theory of multimedia learning, relevant
information in the form of words and pictures is first selected,
then words and images are organized, and finally words and
pictures are integrated by building connections to make sense.
Mayor’s theory gives sound theoretical rationale for the use of
multimedia and CAIs in medical education too; an area where
pictures and videos can address the bulk of the cognitive load
of the medical student.
empirical evidence
Although, low effect size of
‘instructional media’ was previously suggested [6],
recent studies provide evidence in favor of CAIs. Issa, et al.
[7], showed that the cohort of medical students instructed using
principles of multimedia design, scored better than the students
instructed using traditional designs, when evaluated for
immediate retention of knowledge and total scores. In a
follow-up study, the authors showed that the modified condition
group scored significantly better than the traditional condition
group on delayed tests of transfer conducted one week and four
weeks after instruction, and on delayed tests of retention
conducted one week and four weeks after instruction. The
modified condition group participants also performed
significantly better than the traditional condition group on
immediate tests of retention and transfer [8].
In another study [9], multimedia was
used for teaching of gross infective pathogen with a reformed
courseware. Results
showed that compared with non-reform classes, the reform classes
had significant improvements in results [9]. Based upon these
theoretical principles and empirical evidence, it is imperative
that medical educators use multimedia for learning, as medical
education requires a combination of verbal and pictorial
learning [10].
DOES EVERY JINGLE MINGLE?
Though people learn
deeply from combination of pictures and words than anything
singularly, does that mean that any combination of words and
pictures will work? Not exactly. Simply adding pictures to the
words does not guarantee improved learning. This affectively
means that all multimedia presentations are not equally
effective. Only the multimedia instructions designed on the
basis of the principles of human learning are going to provide
meaningful learning [5]. Accordingly, two broad aspects which
one should be conversant with, while designing effective
multimedia presentations are: Science of learning and Science of
Instruction [10].
Science of
Learning: How People Learn
Learning is the
change in the behavior of the learner. Mayer called it as the
“change in the learner’s knowledge attributable to experience”
[11]. For fostering learning, instructors must be aware of ‘how
learning happens’.
For any learning to happen, material
is first selected, then material is organized and finally
material is integrated and connections built with previous
knowledge [5]. Pursuant to the Mayor’s cognitive theory, five
main types of cognitive processes involved in multimedia
learning have been identified viz, selecting words,
selecting images, organizing words, organizing images, and
integrating [10]. One should also take into account the Knowles’
principles of adult learning, which emphasize that adults are
self-directed, have prior experience on which they build-up new
knowledge, and they learn better in safe learning environment
[12].
The role of human memory and its
processing has to be collated with other processes for driving
home the concept of multimedia learning. Humans have three
functional parts of memory – sensory memory, working memory, and
long-term memory [10]. Sensory memory holds exact copy of
information provided for <0.25 seconds. Working memory stores
more processed version of the information provided for <30
seconds, with limited capacity. Long-term memory stores
knowledge for a longer period of time. Sensory and long-term
memory have unlimited capacity. As working memory has limited
capacity, so for effective multimedia learning to happen, people
must be active learners, seeking meaningful learning.
The interplay between functional parts of the human memory and
cognitive processes involved in the multimedia learning has been
depicted in Fig. 1.
 |
|
Fig. 1 Interplay between memory and cognitive
processes for multimedia learning. |
Science of Instruction: How Instructions Work
Instructional methods should be in congruence with the human
learning and knowledge processing system. It is pertinent to
understand how instructions work, before one can design
effective instructional methods and instructions. Same applies
to multimedia instructions and its application in medical
education.
The first step in designing effective instructions is to specify
the instructional objectives and the knowledge change in the
learner [13]. An instructional objective is a statement clearly
specifying – what is to be learnt, how it will be learnt and how
the change in behavior will be assessed. Next in line is
selecting an appropriate instructional strategy, followed by
assessment. Instructional objectives, instructional strategies
and assessment, all should be in alignment. Instructional
objectives, strategies chosen and assessment should also be in
alignment with the specific domain of learning. Well aligned
instructional objectives, instructional methods and assessment,
not in congruence with domain of learning will not lead to
meaningful learning. Overall efforts should be made to create
effective learning environments.
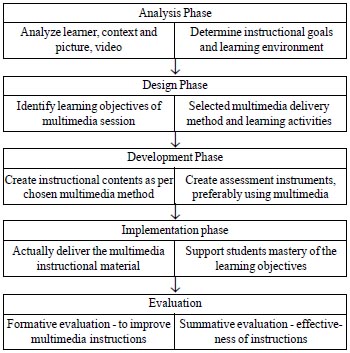
Authors are of the view that for designing multimedia
instructions; analysis, design, development, implementation, and
evaluation (ADDIE) model is best suited as it uses a behavioral
approach in designing instructions [14]. As per this model,
instructional designs pass through five phases of analysis,
design, development, implementation, and evaluation.
In the analysis phase, the existing materials in the form of
pictures, videos, exhibits, X-rays, ultrasounds, etc.
will be analyzed for further use in designing multimedia
instructions. In designing phase, multimedia delivery method
(printed text-figures, power point presentations, computer disc,
webinar, virtual classroom etc.) will be selected, and
then instructional content will be created accordingly in next
phase (Fig. 2). Evaluation in multimedia
instructions is largely confined to two aspects – test of
retention and test of transfer [5]. Performance on these two
aspects can measure learner’s outcome - poor performance on both
types of test indicate no learning; good performance on
retention only indicates rote learning, while good performance
on both types of tests indicate meaningful learning [10]. One
should try to design and use multimedia assessment while using
multimedia instructions, based upon cognitive theory of
multimedia assessment [15].
|
| Fig. 2 Phases
and activities for designing multimedia instructions as
per ADDIE model. |
MOVING FROM THEORY TO PRACTICE
The above mentioned theories and instructional design aspects
make sound foundation for how the faculty members in medical
colleges can design multimedia instructions. Mostly medical
college faculty uses multimedia only for designing power point
(PPT) slides- based instructions and presentations. Other
multimedia contents are mostly made available by software
developers as ‘ready-to-use’ materials. Most of the papers found
in literature have restricted the discussion only about font
type and size to be used in PPT slides, color combinations,
number of lines etc. for making slides better
presentable; in the next section we discuss briefly how
effective PPTs can be designed based upon multimedia
instructions developed through empirical evidences and practical
issues.
After scanning almost 100 studies, Mayer identified 12
principles of developing and designing multimedia instructions
[7,10,16]. These 12 principles have broadly been factorized into
three generic principles in literature viz. curtail
extraneous processing; manage essential processing, and
nurture generative processing [7,10].
Extraneous processing is a type of cognitive processing that
does not support the learning objective, often caused by poor
instructional design, like picture on one slide and its
explanation on another slide of presentation. No doubt, such
processing must be reduced to have less cognitive load.
Essential processing is the process of representing the
essential material to the working memory, through the process of
selecting and organizing. This cognitive processing must be
managed. Generative processing involves the process of making
sense from the presented material through integrating and
organizing. This needs learners motivation and engagement too,
thus generative processing needs to be nurtured. Readers
interested in details of these processes may refer Mayer’s
write-up on the same [17].
These factors along with strategies which can be devised for
effective designing of PPT based multimedia instructions have
been depicted in Fig. 3 [7,10,17].
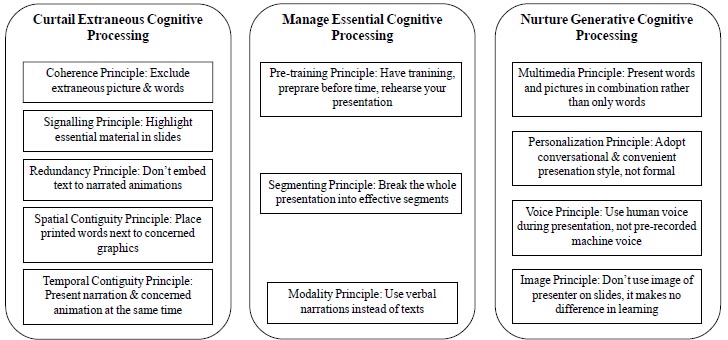 |
| Fig. 3
Principles of
instructional design for multimedia presentations
adapted for effective power-point based presentations. |
Above mentioned principles can be
easily incorporated to make slide presentations interesting,
engaging and effective. In the next section, we have tried to
present graphically the strategies to incorporate major
multimedia instructional design principles for preparing
effective power-point presentations.
Multimedia
principle:
While preparing slides, both words and pictures should be used,
instead of using words alone (Web
Fig. 1). This will also be in accordance with the
‘dual channel’ assumption of the cognitive theory of multimedia
learning.
Coherence
principle:
Do not use unnecessary and unimportant pictures, words and
animations in your presentation (Web
Fig. 1). These unnecessary elements are
bound to increase cognitive load on the learners. Exclusion of
unnecessary elements from slides will also be in accordance with
the ‘limited capacity’ assumption of the cognitive theory of
multimedia learning.
Signalling
principle:
The essential and important material in the slides must be
highlighted (Web Fig.
2). This can be done by using a text box option or by
using the glow text effect.
Contiguity
principle:
Learning from slides is better when pictures and concerned words
are presented near to each other than separated from each other
on a slide (Spatial contiguity). Similarly, learning is better
when pictures and related words are presented simultaneously and
on the same slide rather than successively or on the next slide
(Temporal contiguity) (Web
Fig. 2). This enhances ‘active
processing’, another assumption of the cognitive theory of
multimedia learning.
Segmenting principle:
Presentation should be divided into different effective segments
for better interaction with the content of the presentation and
meaningful learning (Web Fig.
2). Same can apply to one slide, where space must be
used in different sections, if required.
Redundancy principle:
While using an animation in the presentation, don’t overload the
slides / presentation with text also. Narration with animation
makes better learning than animation, narration and text. If
text is used along with animation, it will compete for the
visual channel.
Multimedia presentation tools such as power point outshines in
context to its applicability and feasibility at presenting
knowledge in the form of visual information. The message during
large group interactive sessions having embedded colored
figures, charts, and graphics along with text can be better
conveyed by using multimedia instructional principles while
preparing power point presentations [18]. It has been proven
beyond doubt that adapting powerpoint slides of lectures
according to multimedia principles is likely to translate in to
improved short-term retention among medical students [7].
FACULTY READINESS AND TRAINING
It has been noticed worldwide that the effective use of
educational technology in medical education depends largely upon
faculty readiness, which in turn depends upon faculty training.
Medical faculty must be trained in at least three wider aspects
of educational technology in medical education viz,
understanding of technical operations of the technology,
understanding of the ways to utilize this technology for
teaching-learning, and understanding the ways to utilize the
technology for students’ assessment [1].
Are Faculty Members Trained and Ready?
Traditionally,
medical educators are trained to use clinical settings for
teaching-learning and assessment purposes. There are lot of
differences between clinical setting-based teaching-learning and
computer-based teaching-learning. Both will call, not only for
different teaching styles but also different methods of feedback
and assessment. As mentioned earlier in this paper, faculty
members are most verse with theoretical aspects of the same, but
application part is missing. This calls for shifting our focus
from delivering ‘knowledge’ aspects of the training to
‘competency’ aspect. It is the need of the hour to structure
‘competency-based faculty training programs for using advanced
educational technologies’ in medical education by incorporating
the principles of
cognitive theories of multimedia learning, and principles of
multimedia design.
Conclusion
Cognitive principle
of multimedia learning and principles of instructional designs
need to be practically implemented. These principles must be
used while making power-point presentations for medical
education, so as to make lectures interesting, interactive and
effective. These slight modifications will definitely improve
the retention of the medical students.
Contributors:
TS,PG: conceptualize the paper; RM,KG,SK: wrote the paper;
RM,TS,PG: critically reviewed the paper; RM,KG,SK: revised the
paper. All
authors approved the final version of manuscript, and are
accountable for all aspects related to the study.
Funding:
None; Competing interest: None stated.
References
1. Association of American
Medical Colleges. Effective Use of Educational Technology in
Medical Education - Colloquium on Educational Technology:
Recommen-dations and Guidelines for Medical Educators. Candler
C, ed. AAMC Institute for Improving Medical Education.
Washington, DC: AAMC; 2007.
2. Medical Council of
India. Programme of the revised Basic Course Workshop w.e.f
August 2015. Available from:
https://old.mciindia.org/fdp/8.%20Three%20day%20
revised%20BCW%20programme.pdf. Accessed Septem-ber 6, 2019.
3. Medical Council of
India. Minimum Standard Requirements for the Medical College for
150 Admissions Annually Regulations, 1999 (Amended up to January
2018). Available from:
https://old.mciindia.org/for-colleges/Minimum%20Standard%20Requirements%20
for%20150%20Admissions.pdf. Accessed September 6, 2019.
4. Medical Council of
India. Guidelines for development of skills lab at medical
colleges. Available from:
https://old.mciindia.org/UG-Curriculum/Guidelines
_Develeopment_Skills_Labs_MedicalColleges.pdf. Accessed
September 6, 2019.
5. Mayer RE. Cognitive
theory of multimedia learning. In: Mayer RE, ed.
The Cambridge Handbook of Multimedia Learning. 1st ed.
Cambridge, UK: Cambridge University Press; 2005. p. 31-48.
6. Hattie J. Influences on
student learning. Inaugural Lecture, University of Auckland;
1999. Available from:
https://cdn.auckland.ac.nz/assets/education/
about/research/documents/influences-on-student-learning.pdf.
Accessed October 1, 2019.
7. Issa N, Schuller M,
Santacaterina S, Shapiro M, Wang E, Mayer RE, et al.
Applying multimedia design principles enhances learning in
medical education. Med Educ. 2011;45:818-26.
8. Issa N, Mayer RE,
Schuller M, Wang E, Shapiro MB, DaRosa DA. Teaching for
understanding in medical classrooms using multimedia design
principles. Med Educ. 2013;47:388-96.
9. Zhanga C, Chen X. Use of
Multimedia in Gross Infective Pathogen Experimental Teaching.
Procedia Engineering. 2012;37:64-7.
10. Mayer RE. Applying the
science of learning to medical education. Med Educ.
2010;44:543-9.
11. Mayer RE. Learning and
Instruction, 2nd ed. Upper
Saddle River, NJ: Merrill Prentice Hall Pearson; 2008.
12. Kaufman DM. ABC of
learning and teaching in medicine: Applying educational theory
in practice. BMJ. 2003;326:213-6.
13. Anderson LW, Krathwohl
DR, Airsian PW, Cruikshank KA, Mayer RE, Pintrich P, et al.
A Taxonomy for Learning, Teaching, and Assessing: A Revision of
Bloom’s Taxonomy of Educational Objectives. New York, NY:
Longman 2001.
14. Khalil MK, Elkhider IA.
Applying learning theories and instructional design models for
effective instruction. Adv Physiol Educ. 2016;40:147-56.
15. Kirschner PA, Park B,
Malone S, Jarodzka H. Toward a cognitive theory of multimedia
assessment (CTMMA). In: Spector M, Lockee B, Childress M.
eds. Learning, Design, and Technology. Cham, Switzerland:
Springer; 2016. p. 1-23.
16. Sorden SD. The
cognitive theory of multimedia learning. In: Irby BJ,
Lara-Alecio R, eds. Handbook of educational
theories. Charlotte: Information Age Publishing; 2012. p. 1-31.
17. Mayer RE. Multimedia
Learning. 2nd ed. New York, NY: Cambridge University Press;
2009.
18.Hazari S. Applying instructional design
theories to improve efficacy of technology-assisted
presentations. Journal of Instruction Delivery Systems.
2004;18:24-33.


