Hematopoetic, hepatic and dermatological toxicity of
Carbamazepine is well-known, but cardiac side-effects are
not that widely recognized. Its use has rarely been reported
to cause conduction abnormalities, predominantly in elderly
women, with therapeutic (or moderately elevated) plasma
concentrations of the drug [1]. We herein report a child
with syncopal attacks following carbamazepine use.
An 8-year-old child presented with
history of fainting attacks while playing, which lasted for
a few seconds, followed by spontaneous recovery. He had two
such witnessed episodes in the preceding week, which
prompted the present consultation. He was developing
normally, studied in class III, and never had any previous
episodes of dizziness, syncope, breathlessness or cyanosis.
He did not report any other associated cardiac symptoms. He
was on regular treatment with carbamazepine (15 mg/kg/d) for
Idiopathic generalized epilepsy from another institution
since past one year, with no non-compliance, or missing a
dose in the last 24-hours. Contrast-enhanced CT head done at
that time was normal.
On detailed history, these episodes of
fainting did not resemble the seizures that he had
experienced in the past, and during this episode he did not
have any other neurologic symptoms. The fainting attacks
were transient and the child recovered immediately after the
fall. On examination, the patient was alert and cooperative
with blood pressure of 98/76 mmHg. He was noted to have an
irregularly irregular pulse, and ectopic heart beats after
every 8 to 10 beats, with a heart rate of 70 to 80 beats per
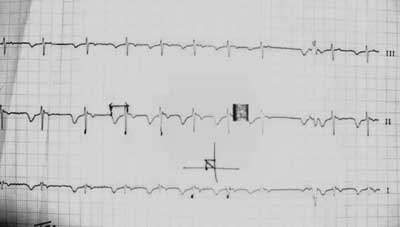
minute. A 12-lead electrocardiogram showed ventricular
premature beats (Fig. 1). Child was admitted
and started on tablet atenolol, 25 mg daily . An
echocardiogram ruled out structural heart disease. Holter
monitoring for 24 hours showed frequent ventricular ectopic
beats though the child did not have further fainting
episodes during the hospital stay.
 |
|
Fig. 1 Ventricular
premature beats seen in the child’s
electrocardiogram on admission.
|
In the background of reports of
carbamazepine causing conduction disturbances, it was
replaced with tablet valproate 15 mg/kg/day. Atenolol was
stopped. Serum carbamazepine level six hour after the last
dose of the drug was 10.6 µg/mL (therapeutic range 8-12 µg/mL).
The patient was discharged on day 5, after documenting a
normal ECG. Repeat holter study at 3 months of follow-up,
did not show any abnormality. On follow-up at one year, he
was asymptomatic without any complaints of fainting attacks
or giddiness.
Carbamazepine exerts its effect by acting
as a sodium channel blocker, and is known to produce
negative chronotropic and dromotropic effects on the heart;
thus, it may sometimes lead to conduction disturbances,
including Sinus bradycardias, sinus pauses, junctional
bradycardias, and AV blocks, ranging from first degree to
complete [2]. A recent review of these reports
showed that elderly women, particularly those with a
pre-existing conduction abnormality, were mostly involved
[1], though reports in young also exist. Usually brady-arrhythmias
occur at therapeutic doses, whereas sinus tachycardia is the
main arrhythmia in massive CBZ overdose [3]. An increase in
ventricular premature beats over next five days has also
been reported in patients who abruptly discontinued CBZ
because of cardiac side-effects [4]. Our patient, however,
did not have any history of discontinuation of the drug
prior to presentation. Another possibility could have been
arrhythmia-related seizures [5]; however, there was no
recurrence of the ECG abnormality after stopping
carbamazepine. Using the Naranjo Adverse Drug Reaction
Probability Scale classified the event as a ‘possible’
adverse drug reaction.
We wish to highlight that cardiac
side-effects may sometimes occur after prolonged
carbamazepine therapy, and may be associated with normal or
slightly high serum levels. As seen in this child, rapid
resolution of symptoms occurs on discontinuing the drug.
1. Hewetson KA, Ritch AE, Watson RD. Sick
sinus syndrome aggravated by carbamazepine therapy for
epilepsy. Postgrad Med J. 1986;62:497-8.
2. Tomson T, Kenneback G. Arrhythmia,
heart rate variability, and antiepileptic drugs. Epilepsia.
1997; 38:S48-51.
3. Kasarskis EJ, Berger R, Nelson KR.
Carbamazepine-induced cardiac dysfunction. Characterization
of two distinct syndromes. Arch Intern Med. 1992;152:186-91.
4. Kennebäck G, Ericson M, Tomson T,
Bergfeldt L. Changes in arrhythmia profile and heart rate
variability during abrupt withdrawal of antiepileptic drugs.
Implications for sudden death. Seizure. 1997;6:369-75.
5. Venugopalan P, Al-Anqoudi ZA, Al-Maamari WS. A child
with supraventricular tachycardia and convulsions. Ann Trop
Paediatr. 2003;23:79-82.


