|
|
Research Papers Indian Pediatrics 2008; 45:463-468 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Central Diabetes Insipidus: Clinical Profile and Factors Indicating Organic Etiology in Children |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
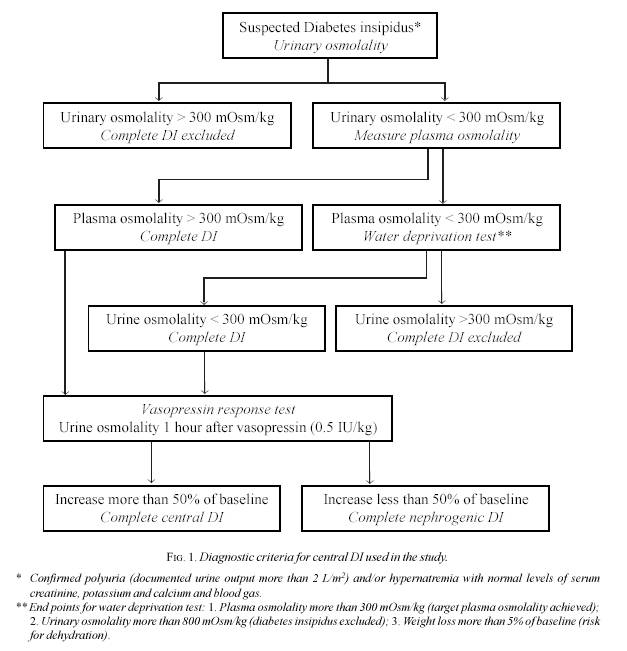
Introduction Central diabetes insipidus (DI) is considered an indicator of serious underlying disease in children(1). Important causes of childhood central DI include tumors and malformations of the central nervous system (CNS), histiocytosis and insults to the hypothalamic-pituitary region by surgery, radiation and trauma(2-8). It is difficult to determine the underlying etiology in a significant proportion (17.5-52%) of children with central DI despite exhaustive evaluation(2-8). While the diagnosis of central DI due to malformation or surgery of CNS and histiocytosis is clear-cut, differentiating idiopathic from organic central DI requires extensive investigations. This is particularly true for CNS tumors such as germinoma, which frequently present without any neurological features. Differentiation of these children from idiopathic central DI is critical, making the identification of pointers to an organic etiology in central DI a desirable goal. There is a paucity of published pediatric data regarding factors indicating organic etiology in central DI(5,6). We undertook this retrospective study to evaluate the profile of children with central DI with special emphasis on identifying factors indicating organic etiology. Methods Case records of children with central DI presenting to the Pediatric Endocrinology Clinic of our hospital from January 1988 to June 2005 were reviewed. The schematic approach to a child with suspected DI (confirmed polyuria and/or hypernatremia after exclusion of other causes) is illustrated in Fig. 1. In children with plasma osmolality less than 300 mOsm/kg (51, 91.3%), water deprivation test was performed after confirming polyuria (urine output more than 2 L/m2 on a 24-hour collection) and exclusion of other causes of polyuria including diabetes mellitus, renal failure, hypokalemia, hypercalcemia and renal tubular acidosis. For water deprivation test, the children were admitted to the day care unit of our hospital in the morning to ensure strict monitoring of hydration status and clinical condition. Water restriction was started after estimation of body weight, hydration status, serum sodium and urinary and plasma osmolality. Subjects were assessed hourly for body weight, hydration status, serum sodium and urinary and plasma osmolality. The test was terminated when urinary osmolality was greater than 800 mOsm/kg, weight loss greater than 5% or plasma osmolality greater than 300 mOsm/kg. Complete DI was diagnosed when urine osmolality remained less than 300 mOsm/kg in the presence of plasma osmolality greater than 300 mOsm/kg. Vasopressin response test was performed in subjects with complete DI to differentiate central from nephrogenic form of DI. Urinary osmolality was measured one hour after intramuscular injection of vasopressin 0.5 IU/kg. Increase in urine osmolality by more than 50% of baseline levels was considered diagnostic of central DI; children with lower increase in urine osmolality were diagnosed as nephrogenic DI(9). Children with plasma osmolality greater than 300 mOsm/kg and urinary osmolality less than 300 mOsm/kg at presentation (5, 8.3%) underwent vasopressin response test without water deprivation. Children with central DI due to brain death were excluded.
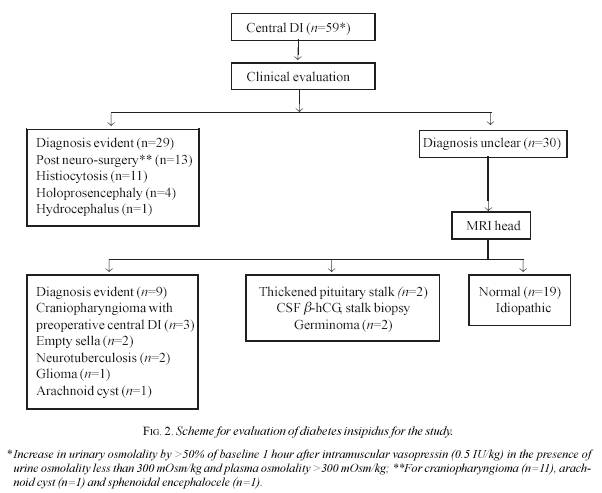
We reviewed the case records for age at diagnosis, family history of disease and clinical features. History of CNS insults including surgery, radiation and infection was recorded. Height was expressed as standard deviation score using the NCHS data(10). Standard deviation score was calculated by the formula [subject’s height – mean height for age] ¸ standard deviation. Detailed clinical examination with special emphasis on CNS involvement, Langerhans cell histiocytosis and midline defects was performed. Magnetic resonance imaging of the hypothalamic-pituitary region, skeletal survey and anterior pituitary evaluation (clonidine stimulated growth hormone, free thyroxine (T4), thyrotropin (TSH), serum cortisol, luteinizing hormone and follicle stimulating hormone) were performed in all subjects. Skin, bone and pituitary stalk biopsy and cerebrospinal fluid b-human chorionic gonadotropin (hCG) levels were done as indicated. Subjects with organic and idiopathic forms of central DI were compared using unpaired student’s t test (for quantitative parameters) and chi square test (for qualitative parameters). Odds ratio was calculated for factors indicating organic etiology and P value less than 0.05 was considered significant. Values are expressed as mean ± standard deviation unless specified. Results Fifty-nine children (40 boys, 19 girls) with central DI were enrolled during the period of study. The mean± SD (range) age at diagnosis was 5.5±3.6 years (4 months to 17 years). Water deprivation test was performed in 54 children with initial plasma osmolality less than 300 mOsm/kg; vasopressin test was done in five children presenting with hypernatremia and plasma osmolality greater than 300 mOsm/kg. In children with post-operative central DI, water deprivation test was done after neurosurgery following the onset of polyuria. Urine output (10±2 mL/kg/hour) was significantly high and in the polyuric range in 54 subjects (91.5%). Presenting features are given in Table 1. TABLE I Clinical Features of Diabetes Insipidus
Etiology: An underlying cause was documented in 40 (67.8%) children. In the two subjects with central DI due to neurotuberculosis, MRI revealed supra-sellar thick walled granulomatous lesions with perifocal edema. MR spectroscopy showed intralesional lipid peaks confirming the diagnosis of neurotuberculosis. Pituitary stalk biopsy and cerebrospinal b-hCG levels confirmed the diagnosis of germinoma in two children with thick pituitary stalk (3.4%). The remaining 19 patients with no obvious abnormality on MRI head were assigned to the idiopathic group (32.2%). MRI head was normal in these children with the exception of absent posterior pituitary hyperintensity in sixteen (84.2%). None of these subjects had ectopic posterior pituitary or thickened pituitary stalk. Children with idiopathic central DI were followed up for 1.9±1.4 years. No neurological feature was noted during follow-up. Follow-up neuroimaging was not performed. Features of children with organic (after exclusion of post-operative form, CNS malformation and histiocytosis) and idiopathic central DI are compared in Table II. All children presenting after the age of five years with growth retardation had an identifiable organic etiology. TABLE II Comparison of Subjects with Idiopathic and Organic forms of Central Diabetes Diabetes Insipidus
*CDI due to Langerhans cell histiocytosis, malformation and surgery of CNS has been excluded. Features of other forms of central DI: Children in the post-operative group were diagnosed at a later age (6.9±4.7 years) compared to those with histio-cytosis (3.7±1.5 years) and CNS malformations (0.4±0.1 years). These children developed perma-nent central DI following removal of cranio-pharyngioma (n=11), sphenoidal encephalocele (n=1) and arachnoid cyst (n=1). Langerhans cell histiocytosis was diagnosed 1.3±0.4 years prior to the onset of central DI in 8 children. Clinical features (seborrhea in 3, skin rash in 2, bone defects in 2 and organomegaly in 1) prompted diagnosis of Langerhans cell histiocytosis in three children. A greater proportion of subjects with post-operative central DI had short stature compared to those with histiocytosis (92.3% against 9.1%, P <0.001). All subjects with CNS malformations had severe developmental delay and were diagnosed as central DI during evaluation for hypernatremia. Discussion The findings of our study suggest that etiological diagnosis is possible in a significant proportion of children with central DI (67.8%), a finding noted in previous studies(4-7). Idiopathic cases accounted for 32.2% in this study, a figure similar to recent reports on childhood central DI (17.9-52%)(4-7). Refinements in diagnostic procedures have resulted in identification of etiology in a greater proportion of children with central DI as exemplified by the diagnosis of CNS germinoma suggested by pituitary stalk thickening in two children without neurological features. The major challenge in the assessment of central DI is to identify those children with organic etiology who require urgent evaluation and management. An etiological diagnosis was possible in 49.2% of our subjects after clinical evaluation. Organic etiology could be established in 36.7% of remaining cases. Neurological features were absent in as many as 54.6% of these cases (two each with germinoma, empty sella and craniopharyngioma). Thus mere absence of neurological signs and symptoms does not rule out an organic central DI. Identification of factors indicating organic etiology of central DI is therefore a desirable goal. In a study of 29 children with central DI, Jaruratanasirikul, et al.(6) observed that presentation after the age of five years was suggestive of organic CDI. Delayed age at onset in organic cases was also observed by Al-Agha, et al.(5) in a study of 39 children with central DI. Growth retardation has been suggested as an indicator of organic CDI(7). Maghnie, et al.(4) however did not observe any difference in the severity of growth retardation in children with organic or idiopathic CDI. In our study older age at diagnosis, short stature and anterior pituitary involvement were indicative of organic etiology. Organic etiology was identified in all children presenting after the age of five years with growth retardation. The generalisability of our study is limited by its small sample size, a factor related to rarity of childhood central DI. There is a need for a multicentric study to evaluate factors indicating organic etiology in children with central DI. An important limitation of our study is the lack of follow-up CNS imaging in idiopathic CDI. Progressive changes signifying evolving CNS neoplasia have been documented in presumed idiopathic CDI(4,5,11). These observations have led to the recommendation of repeated follow-up CNS imaging in children with idiopathic central DI(1). Repeated MRI examinations are often not feasible in resource-poor countries. The pointers to organic etiology (growth retardation, late age at onset and anterior pituitary involvement) may be considered as indications for follow-up neuroimaging under these circumstances. Contributors: AB, MK and PSNM were involved in the management of patients. AB planned the study, collected data, performed the statistical analysis and drafted the manuscript. MK was involved in planning the study and reviewed the manuscript. PSNM was involved in planning the study, critically reviewed the manuscript and would act as the guarantor of the study. Funding: None. Competing interest: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
![]()