|
|
Recommendations Indian Pediatrics 2007;44:443-461 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
IAP Guidelines 2006 on Hospital Based Management of Severely Malnourished Children (Adapted from the WHO Guidelines) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Writing Committee Shinjini Bhatnagar*
Correspondence to: Dr. Shinjini Bhatnagar, Center
for Diarrheal Disease and Nutrition Research, Department of
Pediatrics, All India Institute of Medical Sciences, New Delhi 110
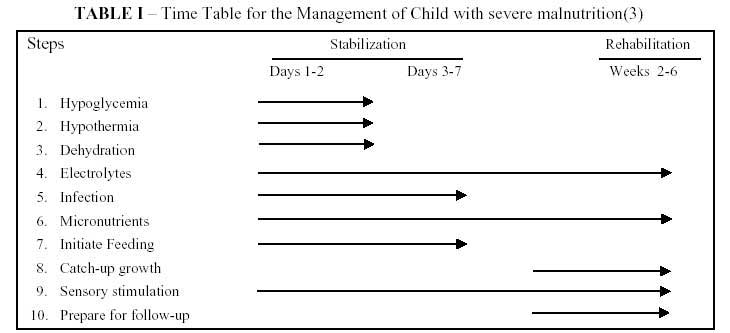
029. 1. Introduction Malnutrition in children is widely prevalent in India. It is estimated that 57 million children are underweight (moderate and severe). More than 50% of deaths in 0-4 years are associated with malnutrition(1). The median case fatality rate is approximately 23.5% in severe malnutrition, reaching 50% in edematous malnutrition(2). There is a need for standardized protocol-based management to improve the outcome of severely malnourished children. In 2006, Indian Academy of Pediatrics under-took the task of developing guidelines for the management of severely malnourished children based on adaptation from the WHO guidelines(3). We summarize below the revised consensus recommendations (and wherever relevant the rationale) of the group. 2. Definition of Severe Malnutrition Severe malnutrition is defined in these guidelines as the presence of severe wasting (<70% weight-for-height or ≤3SD) and/or edema. Mid-upper arm circumference (MUAC) criteria may also be used for identifying severe wasting. The following parameters are associated with an increased risk of mortality: • Weight for height/length <70% NCHS median or ≤3SD. • Visible severe wasting. • Bipedal edema. • MUAC < 11 cm(4). 3. Initial Assessment of a Severely Malnourished Child The initial assessment of a severely malnourished child involves a good history and physical examination. The key points to be covered include history of (i) Recent intake of food and fluids; (ii) Usual diet (before the current illness); (iii) Breastfeeding; (iv) Duration and frequency of diarrhea and vomiting; (v) Type of diarrhea (watery/bloody); (vi) Loss of appetite; (vii) Fever; (viii) Symptoms suggesting infection at different sites; (ix) Family circumstances (to understand the child’s social background); (x) Chronic cough and contact with tuberculosis; (xi) Recent contact with measles and (xii) Known or suspected HIV infection. On examination, it is essential to look for (i) Anthropometry-weight, height/length, mid arm circumference; (ii) Signs of dehydration; (iii) Shock (cold hands, slow capillary refill, weak and rapid pulse); (iv) Lethargy or unconsciousness; (v) Severe palmar pallor; (vi) Localizing signs of infection, including ear and throat infections, skin infection or pneumonia; (vii) Fever (temperature ≥37.5ºC or ≥99.5ºF) or hypothermia (rectal temperature <35.5ºC or <95.9ºF); (viii) Mouth ulcers; (ix) Skin changes of kwashiorkor; (x) Eye signs of vitamin A deficiency and (xi) Signs of HIV infection. 4. Management The current guidelines recommend in-patient management of all severely malnourished children. The treatment guidelines are divided into ten essential steps(1) as shown below: 1. Treat/prevent hypoglycemia 2. Treat/prevent hypothermia 3. Treat/prevent dehydration 4. Correct electrolyte imbalance 5. Treat/prevent infection 6. Correct micronutrient deficiencies 7. Start cautious feeding 8. Achieve catch-up growth 9. Provide sensory stimulation and emotional support 10. Prepare for follow-up after recovery Table I depicts the time-frame for initiating/achieving these 10 steps.
Step 1: Treat/ Prevent Hypoglycemia All severely malnourished children are at risk of hypoglycemia, hence blood glucose should be measured immediately at admission by using glucose estimating reagent paper strips such as dextrostix-reagent strips. There is evidence to suggest association between the hypoglycemia and risk of mortality in severely malnourished children (Table II)(5). TABLE II Association Between Hypoglycemia and Mortality(5)
Diagnosis • Blood glucose level <54 mg/dL or 3 mmol/L is defined as hypoglycemia in a severely malnourished child. If blood glucose cannot be measured, assume hypoglycemia and treat. • Hypoglycemia may be asymptomatic or symptomatic. Symptomatic hypoglycemia manifests as lethargy, unconsciousness or seizures. Sympathetic manifestations of hypoglycemia like pallor and sweating are rare in severe mal-nutrition but may occur. Peripheral circulatory failure and hypothermia may be a manifestation of hypoglycemia. • Hypothermia, infection and hypoglycemia generally occur as a triad. Hence, in the presence of one of these, always look for the others. Treatment If the child has hypoglycemia, but is conscious: • Give 50 mL of 10% glucose or sucrose solution (1 rounded teaspoon of sugar in 3½ tablespoons of water) orally or by nasogastric tube followed by the first feed. (see Step 7 for type and amount of feed). • Start feeding 2 hourly day and night (Initially one can give 1/4th of the 2 hourly feed every 30 minutes till the blood glucose stabilizes). • Start appropriate antibiotics. If the hypoglycemic child is symptomatic (unconscious, lethargic or seizuring): • Give 10% dextrose i.v. 5 mL/kg (if unavailable give 50 mL 10% dextrose or sucrose solution by nasogastric tube). • Follow with 50 mL of 10% dextrose or sucrose solution by nasogastric tube. • Start feeding with the starter F75 diet as quickly as possible and then continue the feeds 2-3 hourly day and night (Initially one can give 1/4th of the 2 hourly feed every 30 minutes till the blood glucose stabilizes). • Start appropriate antibiotics. Monitoring If the initial blood glucose was low, repeat an estimation using finger or heel-prick blood after 30 min. If the blood glucose is again low, repeat 50 mL of 10% dextrose or sucrose solution (as described above). Blood glucose monitoring may have to continue every 30 min till the blood glucose becomes normal and stabilizes; thereafter, start 2 hourly feeding. • In case the body temperature falls (axillary temperature is less than 35ºC or rectal temperature is less than 35.5ºC) or conscious-ness deteriorates measure the blood sugar. Prevention The cornerstone of prevention is feeding at regular intervals. • Feed 2 hourly starting immediately (if necessary, rehydrate first). • Ensure the child is fed regularly throughout the night. Step 2: Treat/ Prevent Hypothermia All severely malnourished children are at risk of hypothermia due to a lowered metabolic rate and decreased body fat. Children with marasmus, concurrent infections, denuded skin and infants are at a greater risk. Always look for and manage hypoglycemia in a hypothermic child. Diagnosis • Hypothermia is diagnosed if the rectal temperature is less than <35.5ºC or 95.5ºF. If axillary temperature is less than 35ºC or 95ºF or does not register on a normal thermometer, assume hypothermia. Use a low reading thermometer (range 29ºC-42ºC), if available. • Hypothermia can occur in summers as well. • Always measure blood glucose and screen for infections in the presence of hypothermia. Treatment • Feed the child immediately (if necessary rehydrate first). • Clothe the child with warm clothes and use a warm blanket. Ensure that the head is also covered well with a scarf or a cap. • Provide heat with an overhead warmer, an incandescent lamp or radiant heater. Do not point the heater directly at the child and avoid contact with hot water bottles, so as to prevent burns. Indirect warming with warm pads could be attempted. • Or the child could be put in contact with the mother’s bare chest or abdomen (skin to skin) as in kangaroo mother care to provide warmth. • Give appropriate antibiotics. Treatment of severe hypothermia (rectal temperature <32ºC) • Give warm humidified oxygen. • Give 5 mL/kg of 10% dextrose IV immediately or 50 mL of 10% dextrose by NG route (if IV access is difficult). • Start IV antibiotics (see section below). • Rewarm: Provide heat using radiation (overhead warmer), or conduction (skin contact) or convection (heat convector). Avoid rapid rewarming as this may lead to dysequilibrium. • Give warm feeds immediately, if clinical condition allows the child to take orally, else administer the feeds through a nasogastric tube. Start maintenance IV fluids (pre warmed), if there is feed intolerance/contraindication for nasogastric feeding. • Rehydrate using warm fluids immediately, when there is a history of diarrhea or there is evidence of dehydration Monitoring • Measure the child’s temperature 2 hourly till it rises to more than 36.5ºC. • Monitor temperature especially at night when the ambient temperature falls and ensure the child is always well covered (particularly the head) and fed on time. • Check for hypoglycemia whenever hypothermia is found. Prevention • Feed the child 2 hourly starting immediately after admission. • Ensure feeds are administered through the night. • Always keep the child well covered. Ensure that head is also covered well with a scarf or a cap. • Place the child’s bed in a draught-free area away from doors and windows to prevent exposure to cold air. • Minimize exposure after bathing or clinical examination. • Minimize contact with wet clothes and nappies and keep the child dry always. • Let the child sleep in close contact with the mother. • The child could also be put in contact with the mother’s bare chest or abdomen (skin to skin) as in kangaroo mother care to provide warmth. Step 3: Treat/Prevent Dehydration Diagnosis Dehydration tends to be over diagnosed and its severity overestimated in severely malnourished children. This is because it is difficult to estimate dehydration status accurately in the severely malnourished child using clinical signs alone. However, it is safe to assume that all severely malnourished children with watery diarrhea may have some dehydration. It is important to recognize the fact that low blood volume (hypovolemia) can co-exist with edema. Treatment Do not use the IV route for rehydration except in cases of shock. The IAP recommends the use of reduced osmolarity ORS with potassium supplements given additionally (Table III). TABLE III Composition of Reduced Osmolarity ORS
Special note: WHO suggests that when using the new ORS solution, containing 75 mEq/L of sodium the ORS packet should be dissolved in two liters of clean water. 45 mL of potassium chloride solution (from stock solution containing 100 g KCl/L) and 50 g sucrose should be dissolved in this solution. These modified solutions provide less sodium (37.5 mmol/L), more potassium (40 mmol/L) and added sugar (25 g/L). IAP Task Force feels that reduced osmolarity ORS without further dilution can be used safely as recommended above, given slowly over a period of 8-10 hours. Extra sugar and potassium can be provided as described in Step 1 and Step 6.
The exact amount depends on how much the child wants, volume of stool loss, and whether the child is vomiting. • Feeding must be initiated within two to three hours of starting rehydration. Give F75 starter formula on alternate hours (e.g., hours 2, 4, 6) with reduced osmolarity ORS (hours 3,5,7) (see Step 7 for volume of feed). Then continue feeding with starter F-75 feeds (see composition Tables VI and VII). TABLE IV Prevalence of Infections in Children with SMN
TABLE V Prevalence of UTI in Children with SMN
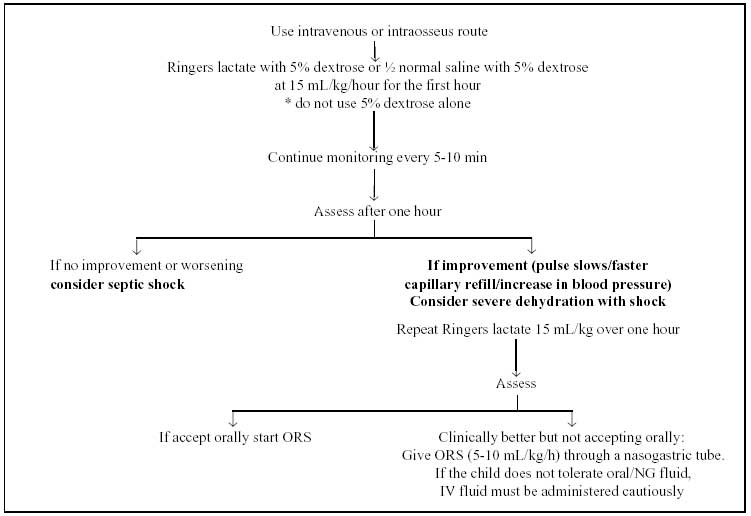
Monitoring Monitor the progress of rehydration half-hourly for 2 hours, then hourly for the next 4-10 hours: • Pulse rate • Respiratory rate • Oral mucosa • Urine frequency/volume • Frequency of stools and vomiting Be alert for signs of overhydration (increasing respiratory rate by 5 per min and pulse rate by 15 per min, increasing edema and periorbital puffiness), which can be dangerous and may lead to heart failure. If you find any sign of overhydration, stop ORS immediately and reassess after one hour. Do not use diuretics in this setting. Decrease in the heart rate and respiratory rate (if increased initially) and increase in the urine output indicate that rehydration is proceeding. The return of tears, a moist oral mucosa, less sunken eyes and fontanelle, and improved skin turgor are also indicators of rehydration; however, these changes may not be seen in some severely malnourished children even when fully rehydrated. Stop ORS for rehydration if any four hydration signs are present (child less thirsty, passing urine, tears, moist oral mucosa, eyes less sunken, faster skin pinch). Prevention Measures to prevent dehydration from continuing watery diarrhea are similar to those for well-nourished children (see Treatment Plan A of management of acute diarrhea), • If the child is breastfed, continue breastfeeding. • Initiate re feeding with starter F-75 formula. • Give reduced osmolarity ORS between feeds to replace stool losses. As a guide, give 50-100 mL (approx. 5-10 mL/kg) after each watery stool. Do not confuse frequent passage of small unformed stools with profuse watery diarrhea; the former does not require fluid replacement. Severe Dehydration with Shock It is important to recognize severe dehydration in severely malnourished children. The management is targeted at replenishment of the intravascular volume by use of intravenous fluids to improve the perfusion to the vital organs. In children with severe malnutrition who present with shock, it may be difficult to distinguish severe dehydration from septic shock. Severely malnourished children must be lethargic/unconscious to be diagnosed with ‘shock’(3). History of profuse watery diarrhea and rapid improvement on intravenous fluids favor the diagnosis of shock due to severe dehydration. Note: A severely malnourished child with signs suggesting severe dehydration but without a history of watery diarrhea should be treated for septic shock. Fluid management for Severe Dehydration (Fig. 1) Intravenous fluids should be given to severely malnourished children if they have signs of shock and are lethargic or have lost consciousness. In case of inability to secure intravenous access, intraosseous route should be used. Ideally, Ringer’s lactate with 5% dextrose should be used as rehydrating fluid. If not available, use half normal (N/2) saline with 5% dextrose. The other alternative is to use Ringer’s lactate solution. • Give oxygen • Give rehydrating fluid at slower infusion rates of 15 mL/kg over the first hour with continuous monitoring (pulse rate, pulse volume, respiratory rate, capillary refill time, urine output). • Administer IV antibiotics. • Monitor pulse and respiratory rates every 10-15 min. If there is improvement (pulse slows; faster capillary refill) at the end of the first hour of IV fluid infusion, consider diagnosis of severe dehydration with shock. Repeat rehydrating fluid at the same rate over the next hour and then switch to reduced osmolarity ORS at 5-10 mL/kg/hour, either orally or by nasogastric tube. • If there is no improvement or worsening after the first hour of the fluid bolus, consider septic shock and treat accordingly.
Caution Do not use 5% dextrose alone Add potassium to the IV fluids at the rate of 1.5 mL per 100 mL after the patient passes urine. There must be frequent monitoring to look for features of over hydration and cardiac decompensation (see Appendix 1 for management of septic shock). Step 4: Correct Electrolyte Imbalance Excess body sodium exists even though the plasma sodium may be low in severely malnourished children. Giving high amounts of sodium could kill the child. In addition, all severely malnourished children have deficiencies of potassium and magnesium; these may take two weeks or more to correct. Edema may partly be due to these deficiencies. Do NOT treat edema with a diuretic. Treatment • All severely malnourished children need to be given supplemental potassium at 3-4 mmol/kg/day for at least 2 weeks. Potassium can be given as syrup potassium chloride; the most common preparation available has 20 mmol/ 15 mL. Note: Wherever it is possible to measure serum potassium and there is severe hypokalemia i.e., serum potassium is <2 mmol/L or <3.5 mmol/L with ECG changes, correct by starting at 0.3-0.5 mmol/kg/hour infusion of potassium chloride in intravenous fluids, preferably with continuous monitoring of the ECG. For arrhythmia attributed to hypokalemia, give 1 mmol/kg/hour of potassium chloride till the rhythm normalizes; this has to be administered very carefully with controlled infusion and continuous ECG monitoring. • On day 1, give 50% magnesium sulphate (equivalent to 2 mmol/mL). IM once (0.3 mL/kg up to a maximum of 2 mL) Thereafter, give extra magnesium (0.4-0.6 mmol/kg daily) orally. Injection magnesium sulphate can be given orally as a magnesium supplement mixed with feeds. • Prepare food without adding salt. Potassium and magnesium can also be supplemented daily by preparing a stock solution of the WHO electrolyte and mineral mix and adding 20 mL of this solution to 1 liter of feed (Appendix 2 for composition). Step 5: Treat/ Prevent Infection In severe malnutrition, multiple infections are common. However, the usual signs of infection such as fever are often absent. Review of literature identifies few studies, mainly from Africa, that have looked at the prevalence of infections in severely malnourished (Table IV)(6-8). In a study from Egypt, 62% of the studied children had lower respiratory tract infection (33% pneumonia, 29% bronchitis). Signs and symptoms were few and mostly non specific in these children. The authors suggested that chest X-ray should be mandatory in evaluating patients with SMN whenever possible(9). Similarly, there are studies that have documented high rates of urinary tract infections in children with SMN (Table V). All these studies showed high rates of infection and majority of the blood stream infections were due to gram negative bacteria. This provides the basis for the recommendation that all severely malnourished children should be assumed to have a serious infection on their arrival in hospital and treated with antibiotics. In addition, hypoglycemia and hypothermia are considered markers of severe infection in children. Investigations In addition to complete clinical evaluation, following investigations may be done for identifying the infections in SMN children, whenever and wherever feasible/available. • Hb, TLC, DLC, peripheral smear • Urine analysis and urine culture • Blood culture • X-ray chest • Mantoux test • Gastric aspirate for AFB • Peripheral smear for malaria (in endemic areas) • CSF examination (if meningitis suspected) Treatment All severely malnourished children should receive broad-spectrum antibiotics Choice of Broad Spectrum Antibiotics Give parentral antibiotics to all admitted children. • Ampicillin 50 mg/kg/dose 6 hourly I.M. or I.V. for at least 2 days; followed by oral Amoxycillin 15 mg/kg 8 hourly for five days (once the child starts improving) and • Gentamicin 7.5 mg/kg or Amikacin 15-20 mg/kg I.M or I.V once daily for seven days. If the child fails to improve within 48 hours, change to IV Cefotaxime (100-150 mg/kg/day 6-8 hourly)/Ceftriaxone (50-75 mg/kg/day 12 hourly). However, depending on local resistance patterns, these regimens should be accordingly modified. If meningitis is suspected, perform lumbar puncture for confirmation, where possible, and treat the child with IV Cefotaxime (200 mg/kg/day 6 hourly) and IV Amikacin (15 mg/kg/day 8 hourly) for 14-21 days. Moreover, if staphylococcal infection is suspected add IV Cloxacillin (100 mg/kg/day 6 hourly). Besides the above, if other specific infections (such as pneumonia, dysentery, skin or soft- tissue infections) are identified, give appropriate antibiotics. Add antimalarial treatment if the child has a positive blood film for malaria parasites. Tuberculosis is common, but anti-tuberculosis treatment should only be given when tuberculosis is diagnosed. Some experienced doctors routinely give metronidazole (7.5 mg/kg 8-hourly for 7 days) in addition to broad-spectrum antibiotics. However, the efficacy of this treatment has not been established by clinical trials. Monitoring It is important to look for response to treatment. The response will be indicated by resolution of the initial symptoms and signs of infection, if any. The child’s activity, interaction with parents and appetite should improve. If there is no improvement or deterioration of the symptoms/signs of infection, the child should be screened for infection with resistant bacterial pathogens, tuberculosis, HIV and unusual enteric pathogens. Prevention of Hospital Acquired Infections The healthcare personnel should follow standard precautions. The effectiveness of hand hygiene should be emphasized to all health care providers, attendants and patients. It is essential that adequate safety measures are taken to prevent the spread of hospital acquired infections, since these children are at higher risk of acquiring infections due to their lowered/compromised immune status. Give measles vaccine if the child is >6 months and not immunized, or if the child is >9 months and had been vaccinated before the age of 9 months, but delay vaccination if the child is in shock. Step 6: Correct Micronutrient Deficiencies All severely malnourished children have vitamin and mineral deficiencies. Micronutrients should be used as an adjunct to treatment in safe and effective doses. Up to twice the recommended daily allowance of various vitamins and minerals should be used. Although anemia is common, do not give iron initially. Wait until the child has a good appetite and starts gaining weight (usually by week 2). Giving iron may make infections worse(14). • Vitamin A orally on day 1 (if age >1 year give 200,000 IU; age 6- 12 m give 100,000 IU; age 0-5 m give 50,000 IU) unless there is definite evidence that a dose has been given in the last month. Give daily Multivitamin supplement containing (mg/1000 cal): Thiamin 0.5, Riboflavin 0.6 and Nicotinic acid (niacin equivalents) 6.6. It is better to aim for a formulation that is truly multi (e.g., one that has vitamins A, C, D, E, and B12 ). • Folic acid 1 mg/d (give 5 mg on day 1). • Zinc 2 mg/kg/d (can be provided using zinc syrups/ zinc dispersible tablets). • Copper 0.2-0.3 mg/kg/d (will have to use a multivitamin/ mineral commercial preparation). • Iron 3 mg/kg/d, only once child starts gaining weight; after the stabilization phase. Step 7: Initiate re-feeding Start feeding as soon as possible with a diet, which has • Osmolarity less than <350 mosm/L. • Lactose not more than 2-3 g/kg/day. • Appropriate renal solute load (urinary osmolarity <600 mosm/L). • Initial percentage of calories from protein of 5% • Adequate bioavailability of micronutrients. • Low viscosity, easy to prepare and socially acceptable. • Adequate storage, cooking and refrigeration. Start cautious feeding • Start feeding as soon as possible as frequent small feeds. Initiate nasogastric feeds if the child is not being able to take orally, or takes <80% of the target intake. • Recommended daily energy and protein intake from initial feeds is 100 kcal/kg and 1-1.5 g/kg respectively. • Total fluid recommended is 130 mL/kg/day; reduce to 100 mL/kg/day if there is severe, generalized edema. • Continue breast feeding adlibitum. Starter diets (adapted from WHO guidelines) recommended in severe malnutrition The diets given below have been adapted for the hospital based Indian settings from the diets recommended in the WHO manual(3). Some examples of diets are given, which could be used to initiate feeding in severely malnourished children. Of these diets, two use cereals in addition to sugar. In addition, older children could be started on cereal-based diets (Table VI). However, there is need for adapting diets using similar concepts in different regional settings in the country. TABLE VI Starter Diets
The cereal-based low lactose (lower osmolarity) diets are recommended as starter diets for those with persistent diarrhea(15). Lactose free diets are rarely needed for persistent diarrhea as most children do well on the above mentioned, low lactose F-75 diets. Children with persistent diarrhea, who continue to have diarrhea on the low lactose diets, should be given lactose (milk) free diets(14). Examples are shown in Appendix 3. How to prepare the feeds? Milk cereal diets do not need cooking, as powdered puffed rice is pre-cooked. Add the sugar and oil to powdered puffed rice. Add the milk and water to prepare the feed. Feeding pattern in the initial days of rehabilitation The volume of feeds should be increased gradually while decreasing the frequency of administration (Table VII). The calories should be increased only after the child is able to accept the increased volume of feeds. TABLE VII Feeding Pattern in the Initial Days of Rehabilitation
Source: WHO guidelines(3). Please see Appendix 4 for the detailed charts on feeding volumes. Step 8: Achieve Catch up Growth Once appetite returns which usually happens in 2-3 days higher intakes should be encouraged. The frequency of feeds should be gradually decreased to 6 feeds/day and the volume offered at each feed should be increased. It is recommended that each successive feed is increased by 10 mL until some is left uneaten. Breast feeding should be continued adlibitum. Make a gradual transition from F-75 diet to F-100 diet. The starter F-75 diet should be replaced with F-100 diet in equal amount in 2 days. These diets as shown below contain 100 kcal/100 mL with 2.5-3.0 g protein/100 mL. The calorie intake should be increased to 150-200 kcal/kg/day, and the proteins to 4-6g/kg/day. Catch-up diets recommended in severe malnutrition The diets given below have been adapted for the Indian settings from the diets recommended in the WHO manual (Table VIII)(2). TABLE VIII Catch-up Diets
Given below are some examples of low lactose catch up diets (Table IX). TABLE IX Low Lactose Catch Up Diet
For children with persistent diarrhea, who do not tolerate low lactose diets, lactose free diet can be started. In these diets, carbohydrates (rice, sugar and glucose) can be given in varying proportions according to the patients’ individual level of carbohydrate to achieve optimal balance between osmolarity and digestibility(15) (see Appendix 5 for an example). Complementary foods should be added as soon as possible to prepare the child for home foods at discharge. They should have comparable energy and protein concentrations once the catch-up diets are well tolerated. Khichri, dalia, banana, curd-rice and other culturally acceptable and locally available diets can also be offered liberally (see IMNCI Food Box)(16). Emergency treatment for severe anemia is shown in Appendix 6, Treatment of associated conditions is shown in Appendix 7. Step 9: Provide sensory stimulation and emotional support Delayed mental and behavioral development often occurs in severe malnutrition. In addition to the above management, try to stimulate and encourage: • A cheerful, stimulating environment. • Age appropriate structured play therapy for at least 15-30 min/day. • Age appropriate physical activity as soon as the child is well enough. • Tender loving care. Step 10: Prepare for follow-up after recovery Primary Failure to respond is indicated by: • Failure to regain appetite by day 4. • Failure to start losing edema by day 4. • Presence of edema on day 10. • Failure to gain at least 5.g/kg/day by day 10. Secondary failure to respond is indicated by: Failure to gain at least 5 g/kg/day for 3 consecutive days during the rehabilitation phase. What is poor weight gain? • Good weight gain is >10 g/kg/day and indicates a good response. It is recommended to continue with the same treatment. • Moderate weight gain is 5-10 g/kg/day; food intake should be checked and the child-ren should be screened for systemic infection. • Poor weight gain is <5 g/kg/day and screening for inadequate feeding, untreated infection, tuberculosis and psychological problems is recommended Possible causes of poor weight gain are:
• That night feeds have been given • That target energy and protein intakes are achieved. Is actual intake (offered minus food left) correctly recorded? Is the quantity of feed recalculated as the child gains weight? Is the child vomiting or ruminating? • Feeding technique: Is the child fed frequently and offered unlimited amounts? What is the quality of care? Are staff motivated/ gentle/ loving/patient? • All aspects of feed preparation: Scales, measurement of ingredients, mixing, taste, hygienic storage, adequate stirring if separating out. • If giving family foods with catch-up F-100, that they are suitably modified to provide >100 kcal/100 g (if not, they need to be re-modified).
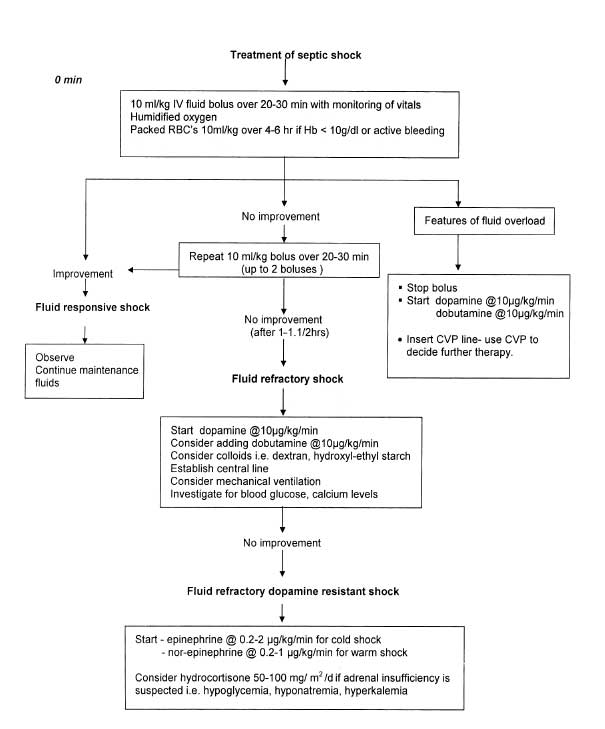
1. Adequacy and the shelf life of the multivitamin composition. 2. Preparation of electrolyte/mineral solution and whether they have been correctly prescribed and administered. (c) Untreated infection If feeding is adequate and there is no malabsorption, infection should be suspected. Urinary tract infections, otitis media, TB and giardiasis are often overlooked. It is therefore important to: • Re-examine carefully. • Repeat urinalysis for white blood cells. • Examine stool. • If possible, take chest X-ray. Antibiotic schedule is modified only if a specific infection is identified. (d) HIV/AIDS In children with HIV/AIDS, good recovery from malnutrition is possible though it may take longer and treatment failures may be common. Lactose intolerance occurs in severe HIV-related chronic diarrhea. Treatment should be the same as for HIV negative children. (e) Psychological problems It is recommended to check for: Abnormal behavior such as stereotyped movements (rocking), rumination (self stimulation through regurgitation) and attention seeking. These should be treated by giving the child special love and attention. Criteria for discharge Severely malnourished children are ready for discharge when the following criteria have been fulfilled: • Absence of infection. • The child is eating at least 120-130 cal/kg/day and receiving adequate micronutrients. • There is consistent weight gain (of at least 5 g/kg/day for 3 consecutive days) on exclusive oral feeding. • WFH is 90% of NCHS median; The child is still likely to have a low weight-for-age because of stunting. • Absence of edema. • Completed immunization appropriate for age. • Caretakers are sensitized to home care. Advise caregiver to: • Bring child back for regular follow-up checks. • Ensure booster immunizations are given. • Ensure vitamin A is given every six months. • Feed frequently with energy-and nutrient-dense foods. • Give structured play therapy. Criteria for discharge before recovery is complete is shown in Appendix 8. The data were presented at a workshop conducted under the aegis of WHO, India and UNICEF to the other members of the Task Force (Appendix 9) in May 2006. Acknowledgements We acknowledge UNICEF and WHO India Office for technical and financial support for the meeting and adopting the guidelines. If the patient is considered to have septic shock: • Continue administration of oxygen. • Give 10 mL/kg Normal Saline or Ringers’ Lactate bolus cautiously over 20-30 minutes. Repeat boluses till a total of 30 mL/kg of crystalloids. This fluid administration rate is much slower than what is currently recommended for children(4). • Consider colloids i.e., high molecular weight dextran, degraded gelatin, hydroxyl-ethyl starch etc, when 30 mL/kg crystalloids have been used and more fluid infusion is required. • Monitor vitals, urine output, sensorium, features of fluid overload and cardio-respiratory status during boluses to monitor the response to fluid therapy and then at least hourly (more frequently if required). • Stop bolus and restrict fluids/colloids at first sign of fluid overload (appearance of crepitations or S3, worsening respiratory distress, increase in liver size). • Consider Central Venous Pressure (CVP) monitoring to guide fluid therapy in fluid refractory shock, wherever feasible. • Consider mechanical ventilation in fluid refrac-tory shock to decrease work of breathing (This may be feasible in only some health care settings). • Start vasoactive agents, dopamine (10-20 µg/kg/min), dobutamine (10-20 µg/kg/min) as indicated (see flow chart). Adjust the dose according to the response. • Consider 10 mL/kg packed red blood cells slowly over 4-6 hours if hemoglobin is <10 g/dL or the patient is actively bleeding. • Use appropriate and adequate antibiotics: Third generation cephalosporins and aminoglycosides should be added within 1st hour of shock. Add antistaphylococcal cover if indicated.
If available, also add selenium (0.028 g of sodium selenate, NaSeO4 10H2O) and iodine (0.012 g potassium iodide, Kl) per 2500 mL. • Dissolve the ingredients in cooled boiled water. • Store the solution in sterilized bottles in the fridge to retard deterioration. Discard if it turns cloudy. Make fresh each month.
Appendix 1 Treatment of septic shock (see flow chart below)
(Adapted from: Carcillo JA, Fields AI. American College of Critical Care Medicine Task Force Committee Members. Clinical practice parameters for hemodynamic support of pediatric and neonatal patients in septic shock. Crit Care Med 2002; 30: 1365-1378).
Appendix 2 Composition of concentrated electrolyte/ mineral solution:
Appendix 3 Starter lactose free diet Lactose free diets are rarely needed as most children do well on the above mentioned, low lactose F-75 diets.
* Egg white may be replaced by 3g of chicken or commercially available pure protein like casein.
**Powdered puffed rice may be replaced by commercial pre-cooked rice preparations (in same amounts).
Appendix 4 Volumes of F-75 per feed (approx 130 mL/kg/day)
Appendix 5 Catch-up lactose free diet
Appendix 6 Emergency Treatment
Appendix 7 Treatment of Associated Conditions
(NB: Children with vitamin A deficiency are likely to be photophobic and have closed eyes. It is important to examine the eyes very gently to prevent rupture). Appendix 8 Discharge Before Recovery is Complete
Appendix 9 Members of the Task Force
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()