|
|
Images in Clinical Practice Indian Pediatrics 2006; 43:549 |
||
|
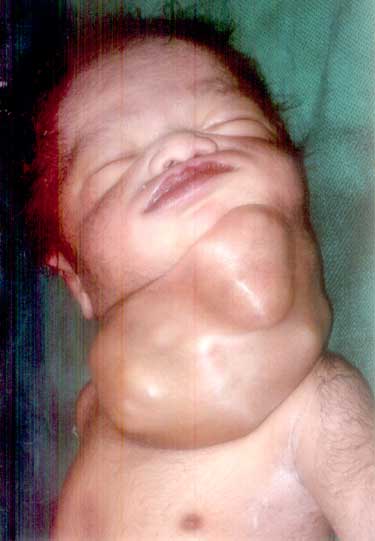
Congenital Cervical Teratoma |
||
|
Cervical teratomas account for approximately 3% of neonatal teratomas. The histologic appearance of these masses is varied because all three germinal layers are represented. Often immature neural elements are identified, especially in the solid portion of the tumor, suggesting neuroectodermal origin. Airway compromise is the most serious postnatal complication of giant cervical teratoma, and prenatal diagnosis is crucial, allowing for early recognition of neck masses that obstruct the airway. A prenatal ultrasound can identify the characteristic appearance of multiloculated cystic mass originating most commonly from the anterolateral aspect of the fetal neck. Polyhydroamnios and rarely non-immune hydrops are associated with this condition. The other conditions that need to be considered for a mass at this site include cystic hygroma (usually transilluminant), cervical goiter, cervical sarcomas and neuroblastoma. Management strategies for giant cervical teratomas include in-utero resection, resection on placental support during an ex-utero intrapartum treatment (EXIT) procedure, intubation or tracheostomy during EXIT, and postnatal resection. Prerna Batra,
|
![]()