|
|
Brief Reports Indian Pediatrics 2006;43:527-534 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Neurodevelopmental Assessment in the First Year with Emphasis on Evolution of Tone |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sudha Chaudhari and Bhushan Deo From the Department of Pediatrics, King Edward Memorial Hospital, Pune 411 011, India. Correspondence to: Dr. Sudha Chaudhari, Consultant, Division of Neonatology, Department of Pediatrics, KEM Hospital, Pune 411 011. E-mail kemhrc@vsnl.com Manuscript received: July 8, 2005, Initial review
completed: September 20, 2005;
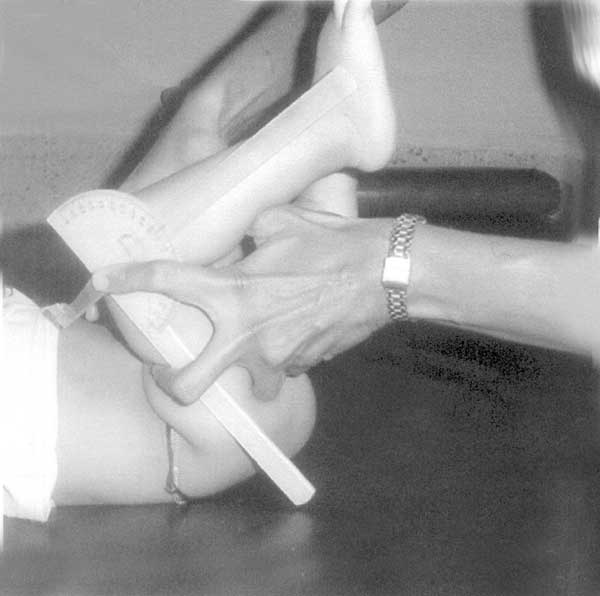
Changes in neuromotor function observed during the first year of life are closely related to the maturation of the central nervous system and the presence or absence of brain damage. Hence it is important to detect abnormalities in neurodevelopment as early as possible, so that intervention programmes can be started(1). Saint-Anne-Dargassies(2) described assessment of tone as an important aspect of neurodevelopmental evaluation. Muscle tone is difficult to define. It is that condition of the muscle determined by physical, chemical and nervous influences, which determine body posture, the range of movements at joints and the feel of the muscle(3). Passive tone indicates extensibility of a muscle. It is observed by a maneuver evaluating the amplitude of a slow movement executed by the observer, with the infant remaining passive. The result is expressed as an angle or in relation to a landmark (scarf sign). The waxing and waning pattern of tone was described by Amiel-Tison based on the work of Dargassies(4). The passive tone increases in a caudocephalic fashion from 28-40 weeks, so that a term infant is born with maximum physiological hypertonia and the muscle tone then decreases in a caudocephalic manner in the first year(5). On the other hand, active tone progresses in a cephalo-caudal fashion from birth to 12 months, so that head support comes first at 3 months and standing with support comes at 9 months. Various influences, genetic, racial, may play a role in determining passive tone. The values described in Caucasian French infants may not hold true for Indian infants. The main aim of this study was not only to assess neurodevelopment in normal infants, but to evaluate the changing measurements of passive tone in the form of various angles in the first year of life. Subjects and Methods One hundred normal infants discharged from the Obstetric ward of a teaching hospital within a six month period, were enrolled in this prospective study. The inclusion criteria were: (i) gestational age >37 weeks; (ii) birth weight >2500 g; (iii) normal antenatal and perinatal course; and (iv) normal delivery. The exclusion criteria were: (i) presence of congenital anomalies or (ii) neurologic illness during the 12 month followup. The mothers were informed about the project and their consent was taken. The infants were examined 24 hours after birth. Their weight, length, head circumference was recorded. Clinical examination was done to rule out any obvious congenital anomaly. Cry, suck, activity and primitive reflexes were noted in order to rule out any neurologic damage. Every effort was made to get a good follow up. The social worker gave dates of scheduled appointments and a letter was sent one week prior to the appointment. If an appointment was missed, a home visit was made to find out the cause of attrition by the social worker. Socio-economic status was determined by the Kuppuswamy Scale(6). All the infants were seen in the Well Baby Clinic every month. However, formal neuro-developmental assessment was done at 3, 6, 9, 12 months. At every visit, a detailed anthropometry was recorded. Weight, height, head circumference were plotted on a growth chart to ensure that there was no growth faltering. Nutritional advice and immunization was given. If the infant was ill on the day of testing, the testing was postponed. However, if an infant came 7 days after the pre-determined appointment, the testing was not done. A neurodevelopmental screening test developed in our department and validated on 150 normal infants in our Well Baby Clinic was used. Tools used A. Neurodevelopmental assessment (i) A red ball for visual fixation and pursuit. (ii) (a) A ‘pooja bell’ to test hearing at 3 months. (b) A piece of paper - crackling of paper at 6 months(iii) A red rattle and red pen to test mouthing, voluntary reach and transfer of objects. (iv) A coloured paper clip to test for pincer grasp. (v) A paper and pen to see for scribbling (imitative or spontaneous) at one year. B. Evaluation of passive tone Goniometer: This is a metallic, non-traumatic portable instrument used for measuring angles. It consists of two arms attached with a screw. On one arm, a protractor is fixed, which is calibrated upto 180 degrees. The infant was assessed in a quiet room, when he or she was not hungry, sleepy, irritable or sick. Neurodevelopmental assessment: (1) Examination of head; (2) Neurosensory evaluation- visual fixation and pursuit were tested by a red ball. Hearing was tested by a pooja bell at 3 months and crackling of paper at 6 months; (3) primitive reflexes - palmar grasp, automatic walking, Moro and asymmetric tonic neck reflex at 3 months and protective reflexes like lateral propping and parachute at 9 months; (4) Motor milestones - head support, sitting, crawling, pincer grasp and standing were recorded; (5) Evaluation of tone was done as resting posture, passive tone and active tone. Spontaneous posture was observed by inspecting the child while he lies undisturbed. Passive tone was evaluated by applying certain maneuvers to the infant while he remains passive at rest. These maneuvers must be performed slowly, gently, and just to the point of discomfort. The resistance of an extremity to this manipulation was measured by recording the angle formed at the joint by this movement, using a goniometer (Fig. 1). The following angles were measured.
(i) Angle at hip: Adductor angle. (ii) Angle at knee: Popliteal angle. (iii) Angle at ankle: Dorsiflexion angle. The angle was measured using a slow and a quick movement. A difference of less than 10 degrees between the slow and quick angle was considered as normal. The angles were expressed both as mean (SD) and as ranges. These ranges were then compared with those described by Amiel-Tison. Active tone was studied with the infant moving spontaneously in response to a given stimulus like head support, pull to sit, pull to stand. One testing with Bayley Scales of Infant Development was done during the follow-up, at 6, 9 or 12 months(7). A mental and motor quotient ³85 was considered as normal. Statistical analysis: The data was fed to the computer and analysed using statistical package for social sciences (version 10.0). Mean and standard deviations were determined. Results Baseline data: One hundred full term infants were prospectively followed up for a period of one year. There were 56 males and 44 females in this cohort. Seventy two infants weighed between 2500-3000 g and 28 infants weighed more than 3000 g. Seventy three (73%) infants belonged to the middle class, twelve infants were from the higher class and 15 infants belonged to the lower class. Only 35% of the infants lived in nuclear families and 65% lived in joint families. During the follow up, three infants developed neurologic problems, and were excluded after 6 months. Three families had moved away. Seven babies did not keep their appointments either due to illness or family problems. So at 9 months, only 87 babies and at 12 months, 88 babies were assessed. Eighty five babies came for all the four assessments. Height, weight and head circumference was within ±2 SD on the growth curve in all the babies. Neurodevelopmental assessment (i) Examination of head was normal in all infants. (ii) Visual fixation and pursuit was present in all infants by 3 months of age. (iii) Hearing: All babies were able to turn towards sound at 3 months (100%). At six months, all babies responded to the crackling of paper by turning the head and eyes towards the sound (100%). (iv) Primitive reflexes: Automatic walking, palmar grasp, Moro and asymmetric tonic neck reflex had disappeared at 3 months in all infants (100%). (v) Protective reflexes: The lateral propping reflex had appeared in all 87 infants at 9 months (100%). The parachute reflex had appeared in 84 of the 87 infants (96.5%), at 9 months. (vi) Milestones: All the salient motor and mental milestones and their age of appearance is shown in Table I. Social smile had appeared by history at 6 weeks in all the infants. Table I Age of Appearance of Milestones
(vii) Passive tone: The adductor and popliteal angles were measured with a goniometer (Fig.1). The values of these angles at all the four ages, expressed as mean and standard deviation are shown in Table II. The difference in the slow and quick dorsiflexion angle was less than 10 in all infants at all four testings. Table II shows the adductor, popliteal and dorsi-flexion angles and the scarf sign in the study group. The same angles described as ranges by Amiel-Tison (6) are shown alongside. The angles described by the French group are wide ranges, hence no statistical test could be applied for comparison. Table II
Angles expressed in degrees. (viii) Active tone: There was no head lag at 3 months in all 100 infants (100%). Pull to sit was present in 89 out of 95 infants tested at 6 months (95%). Pull to stand was present in all 87 infants at 9 months (100%). Thirty six infants were assessed at 6 months, thirty five were assessed at 9 months and twenty four were assessed at 12 months by the Bayley Scales of Infant Development. All the infants had a motor and mental quotient >85. Discussion The study of normal development has been a subject of great interest for many researchers. In fact, Charles Darwin published a detailed account of the development of one of his ten children, way back in 1877. Any study in neurodevelopment has to be longitudinal in nature and assessment of tone is an integral part of neuromotor examination. Most conventional neurological assessment tests do not emphasize this aspect. Evaluation of tone must not only be quick and easy, but also standardized. Passive tone is assessed more accurately than active tone because it is independent of strength. It is determined by resting posture, angle of flexion, resistance to extension and passive recoil(8). With improved survival of ‘high risk’ newborns in the last two decades, more and more follow up clinics are coming up and the Amiel-Tison method of neurologic assessment is gaining popularity for planning interventional therapy as well as for prediction. We(9) found the 3 month assessment by this method to be a good predictor of outcome at 12 months. Nair(10) feels that Amiel-Tison has provided us with a comprehensive system of neurologic evaluation. Several authors have used the Infant Motor Screen for early prediction(11). Singhi, et al.(12) reported that they found the Infant Motor Screen to be highly specific for early diagnosis of cerebral palsy. We(13) found the Amiel-Tison neurological test to be more sensitive in detecting abnormal motor development at 3, 6, 9 months compared to the Bayley Scales of Infant Development, but lost its advantage over BSID at 12 months. Reade(14) measured the popliteal angle in 130 normal infants using a goniometer to demonstrate the decreasing limitation of knee extension in the first 8 months of life, way back in 1984. Katz, et al.(15) used the goniometer to measure the popliteal angle in normal children. Kato, et al.(16) studied the evolution of the popliteal angle in the first year of life in five different birth weight categories. They concluded that muscle tone of lower extremities was higher in babies, with birth weight less than 2000 g at 4 months (corrected age) and cautioned against jumping to a conclusion of spastic cerebral palsy. The same authors studied the popliteal angle in infants with periventricular leucomalacia and found a high specificity and positive predictive value at 8 and 12 months for outcome(17). A study from Chandigarh(18) found restricted popliteal angle in 64% of high risk infants, who later developed cerebral palsy. We used the goniometer to measure the angles in order to get a more objective evaluation, since visual measurements are more subjective. We have also expressed the angles as means with standard deviation, so that other centres could compare their results with our values. As far as the dorsiflexion angle is concerned, it is not the actual angle that is important, but the difference between the quick and slow angle is important. Normally, the quick and slow angles are equal. A difference of more than 10 degrees indicates a powerful stretch reflex due to hypertonicity. We have not measured the heel to ear angle as this angle is difficult to elicit and the maneuver is uncomfortable for the infant. We have also confirmed the appearance of many milestones in normal Maharashtrian infants. Social smile had appeared in all infants by 6 weeks, much earlier than that reported by Illingworth(9). It is not surprising as our infants have so much social contact with relatives and grandparents and 65% our babies lived in joint families. Transfer of objects appeared at 6 months, a month earlier than that reported by Illingworth(9). In a country like India, where a regular monthly follow up is not possible to study the evolution of tone, only a single examination may be available. Hence, we felt that it was necessary to evaluate these angles at various ages in the first year of life in healthy infants, to provide normative data of passive tone. Contributors: SC conceived the project, supervised it and wrote the manuscript. BD collected the data. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1. Farber JM, Shapiro BK, Palmer FB, Capute AJ. The diagnostic value of neurodevelopmental examination. Clin Pediatr 1985; 24: 367-372. 2. Saint-Anne-Dargassies S. Le de’velopment neurologique du nouveune’ a’ terme et premature’ 2nd edn. Masson Paris 1974; 6-10. 3. Illingworth RS. The development of the infant and young child 9th edn. London: Churchill Livingstone 1987; 224-225. 4. Amiel-Tison C, Grenier A. Neurological Assessment during first year of life. New York. Oxford University Press, 1986; 46-94. 5. Amiel-Tison C. A method for neurologic evaluation within the first year of life. In: Meyer L, ed. Current Problems in Pediatrics. VII No. 1. Chicago: Year Book Publishers, 1976; 1-50. 6. Kuppuswamy B. Manual of Socio-Economic Status Scale. New Delhi. Manasayan. 1991. 7. Phatak P. Mental and Motor Growth of Indian Babies (1-30 months). Final Report. Baroda: Department of Child Development, MS University , Baroda. 1970. 8. Illingworth RS. The Normal Child. 9th edn. Edinburgh, Churchill Livingstone. 1987; 156-159. 9. Chaudhari S, Kulkarni S, Pandit AN, Koundinya UK. Neurological assessment at three months as a predictor for development in high risk infants. Indian Pediatr 1993; 30: 528-531. 10. Nair MKC. Early interventional therapy editorial. Indian J Pediatr 1992; 59: 657-659. 11. Nair MKC, George B, Mathews S, Lakshmi S, Philip E. Early intervention program for high risk babies: Use of Infant Motor Screen. Indian J Pediatr 1992; 59: 687-690. 12. Singhi P, Radhika S, Bhakoo ON. Use of the infant motor screen for detection of cerebral palsy. In: Scientific Abstracts 8th Asian Congress of Pediatrics & XXXI National Congress of IAP. Chaudhury P, Sachdev HPS, Puri RK, Verma IC (eds.). New Delhi. Jaypee Publishers Ltd; 1994; p. 52. 13. Chaudhari S, Shinde SV, Barve SS, Dixit H, Pandit AN. A longitudinal follow up neuro-development of high risk newborns–a comparison of Amiel-Tison’s method with Bayley Scales of Infant Development. Indian Pediatr 1990; 27: 799-802. 14. Reade E, Han L, Hallum A, Lopopolo R. Changes in popliteal angle measurements in infants upto one year of age. Dev Med Child Neurol 1984;26: 774-780. 15. Katz K, Rosenthal A, Yosipovitch A. Normal ranges of popliteal angle in children. J Pediatr Orthop 1992; 12: 229-231. 16. Kato T, Okumara A, Hayakawa F, Itomi K, Kuno K, Watanabe K, et al. Popliteal angle of low birth weight infants during first year of life. Pediatr Neurol 2004; 30: 244-246. 17. Kato T, Okumara A, Hayakawa F, Itomi K, Kuno K, Watanabe K, et al. Popliteal angle in preterm infants with periventricular leuco-malacia. Pediatr Neurol 2005; 32: 84-86. 18. Radhika S, Singhi P, Walia BNS. Early developmental and psychoactive predictors of cerebral palsy in high risk infants. PhD Thesis data PGIMER. 1991. |
![]()