|
|
Original Articles Indian Pediatrics 2004; 41:551-558 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
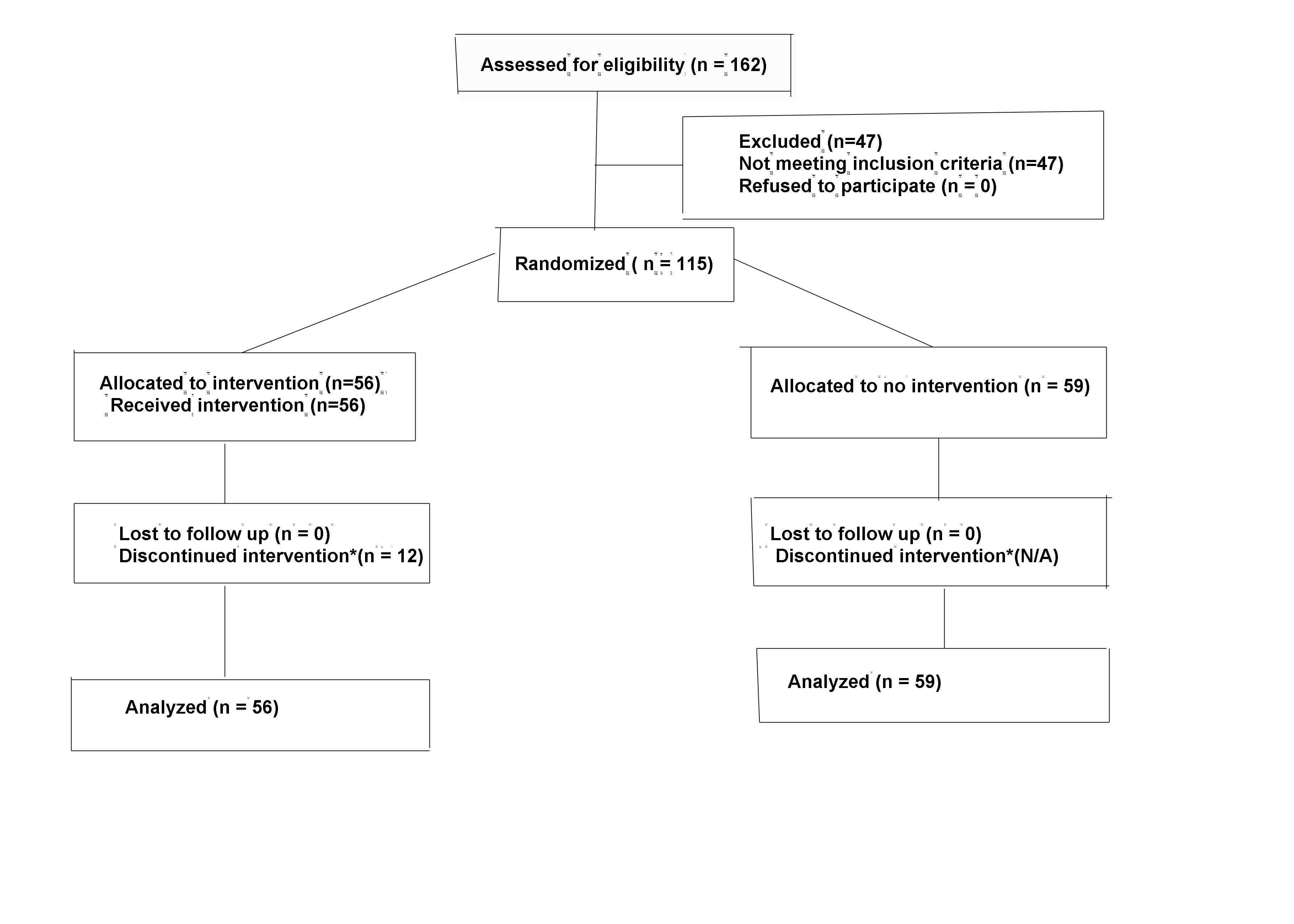
To study the efficacy and complications of low dose indomethacin in the reduction of major intraventricular hemorrhage (IVH) in very low birth weight (VLBW) babies. Design: prospective randomized controlled trial (interim analysis) Setting: Level III neonatal intensive care unit of a perinatal tertiary care center. Patients: Newborn babies with birth weights between 750-1250 g were randomized into indomethacin or control groups. They were further stratified into two birth weight groups 750-999 g and 1000-1250 g for subgroup analysis. Interventions: 3 doses of indomethacin were administered to the indomethacin group at the dose of 0.1 mg/kg/dose intravenously. The control group did not receive any specific intervention other than standard neonatal intensive care. Outcome measures: The primary outcome measure was the occurrence of IVH and the secondary outcome measures were necrotising enterocolitis, symptomatic patent ductus arteriosus (PDA), bleeding episodes, renal failure, chronic-lung disease and death. Results: Out of 115 eligible newborn babies, 56 babies received indomethacin and 59 were controls. Perinatal characteristics were similar between the two groups. There was no difference in the incidence of IVH between the groups but on subgroup analysis the incidence of major IVH (grades III and IV) were significantly increased in babies in the lower birth weight category who received indomethacin (P = 0.03). The incidence of chronic lung disease was significantly higher in the indomethacin group (P = 0.005) and bleeding episodes other than IVH were also significantly increased in the indomethacin group (P = 0.04) in the lower birth weight category. The incidence of PDA was lower in the indomethacin group but only reached significant level in the higher birth weight subgroup (P = 0.02). There were no significant differences in the other outcome measures studied. Conclusions: Indomethacin prophylaxis did not confer protection against IVH in very low birth weight babies. Instead it showed an increase in the risk of IVH, other bleeding episodes and chronic lung disease. Based on this data we felt that we were not ethically justified in continuing the use of indomethacin and have since terminated this study. INTRAVENTRICULAR hemorrhage (IVH) continues to remain a significant cause of long term morbidity among very low birth weight infants(1). Prophylactic low dose indomethacin has emerged as a useful modality in decreasing the incidence of severe grades of IVH borne out by systematic review and meta-analysis of randomized control trials(2). However, most of the data is from Caucasian or African American infants. There is no data to the best of our knowledge on Asian Arab infants. Although the role of prophylactic treatment with indomethacin is now well established, its effect in the subgroup of extremely low birth weight (<1000 g) infants have not yet been examined in detail. Indomethacin is a drug whose pharmaco-dynamics in preterm neonates has been extensively studied and lack of significant adverse effects and efficacy for closure of patent ductus arteriosus (PDA) is well established(3,4). We initiated this prospective, randomized controlled study to assess the efficacy and possible adverse effects of early low dose indomethacin prophylaxis on the incidence of major IVH in very low birth weight babies of Asian-Arab origin. Subjects and Methods This study was conducted at the Neonatal Intensive Care unit of Royal Hospital, Oman from March 1998 and terminated prematurely after three years in March 2001. Inclusion criteria were as follows: 1. Babies born at this institution and who had antenatal care at our facility. 2. Birth weight between 750 g and 1250 g. 3. Absence of major congenital anomalies. 4. Informed consent. 5. Absence of intraventricular hemorrhage prior to randomization. The following babies were excluded: 1. Gestational age <26 weeks. (At present as a policy we are not offering ventilatory support to such babies). 2. Severely asphyxiated at birth (Apgar score <5 at 5 minutes). 3. Chromosomal aberrations. 4. Evidence of intrauterine or intrapartum sepsis on initial investigations. 5. Hematological or renal profiles contra-indicating indomethacin administration. Randomisation Simple random sampling method was used. Sampling frame was created by listing the study units as either cases or controls and numbered. Opaque sealed envelopes containing cards with treatment assignments were then mixed thoroughly and kept in a box under lock. Units were then selected from this sampling frame until the estimated sample size was obtained. This box was opened by the in charge nurse on shift when a baby was admitted and identified for the study, and the registrar on call drew an envelope. Indomethacin was administered to the cases at the dose of 0.1 mg/kg/dose intra-venously over a period of not less than 30 minutes between 6 to 12 hr of age. The first cranial ultrasound was done before randomization. Two additional doses were administered at 24 hr intervals if the initial ultrasound had detected no IVH. The medication was discontinued if any of the following was detected: IVH more than grade II, necrotizing enterocolitis, pulmonary hemorrhage, gastrointestinal bleed or bleeding from puncture sites, platelet count <50,000 cumm, serum creatinine >160 µmol/L, sodium <120 or >150 mEq/L, potassium >7 mEq/L and urine out put <0.5 mL/kg/hr. The control group did not receive any specific intervention other than standard neonatal intensive care as per the protocols of the Unit. Outcome Measures The primary outcome measure was the occurrence of IVH. Secondary outcome measures studied were the occurrence of necrotizing enterocolitis, symptomatic PDA, bleeding episodes, renal failure, chronic lung disease and death. Ultrasound examination was done using ultrasound machine (Model-Toshiba Sonolayer–VssA-90A) using a 7.5 MHz transducer. IVH was graded according to Papile, et al.(5). Periventricular leukomalcia (PVL) was identified as echodense intra-parenchymal lesions located at the external angles of lateral ventricles and more echodense than the choroid plexus. The following monitoring were done on all babies: (a) Ultrasound on days 1,3 and 7 and weekly thereafter till discharge or death. (b) Blood urea, creatinine, electrolyte and platelet count daily for the first four days, as is the standard policy in our Unit. (c) Strict intake output charting. Adverse events like necrotizing entero-colitis, chronic lung disease, PDA, renal failure, bleeding episodes, etc. were diagnosed as per standard definitions in neonatal practice. Echocardiography was done by pediatric cardiologist, on all babies who developed a cardiac murmur. PDA was considered symptomatic if there was hemorrhagic pulmonary edema, cardiomegaly on chest x- ray, or failure of weaning from ventilatory support. Asymptomatic PDA in preterm babies is not treated in our setting. A second course of indomethacin was given to babies who developed symptomatic PDA if they did not respond to fluid restriction for 48 hr. None of these babies had to undergo PDA ligation. All the treatment modalities like mechanical ventilation, surfactant administration, fluid and TPN administration, enteral nutrition and drugs were as per the protocols in the Unit and were applied to all babies. Statistical Methods Analysis of our data from the years prior to 1998 had shown an incidence of 15% in major grades of IVH in babies with birth weight below 1251 g. Sample size calculation to reduce major IVH from 15% to 5% with an alpha value of 0.05 and a power (1-beta) of 0.85 estimated that 154 babies would be required in each limb of the study. We have a delivery rate of about 5000 per year. About 1.5% of our hospitals born babies are £1250 g at birth. At this rate it would have taken us approximately six years for recruiting adequate number of eligible babies. Hence, an interim analysis at 3 yr or when 50% recruitment was obtained, was planned at the outset itself. Categorical data was analyzed using the Chi Square test for proportion; Fisher exact test was used if a cell value was less than 5. Epi Info 6 statistics program was used for sample size estimation, power and calculation of relative risk (RR). The research and clinical studies committee of the Royal Hospital approved the study. Results The detail of the progress of the study is shown in the flow diagram (Fig. 1). During the three year period a total of 162 babies were born with weight in the range of 750-1250 g; 115 of them were eligible and informed consent was obtained. After randomization 56 babies received indomethacin and the rest 59 were controls. They were further subdivided into two birth weight categories 750-999g and 1000-1250 g in each limb for analysis.
Fig. 1. Flow diagram of subjects progress through the study. * See text for reasons All perinatal characteristics of the babies at study entry were evenly matched between both the groups (Table 1). There was no significant difference between the two groups in the incidence of all grades of IVH respectively. However, on subgroup analysis ( Table II), there was a significantly increased incidence of major IVH amongst the babies who received indomethacin in the lower birth weight subgroup (P = 0.03, RR 2.05, 95% CI 1.29-3.26). One baby who received indomethacin amongst the lower birth weight subgroup did not have IVH initially but showed PVL on subsequent ultrasound scanning. There was a natural decline in the incidence of major grades of IVH during the study period - 4 babies out of 59 controls (6.8%) compared to 15% in the three years prior to the study period.Table I Clinical Characteristics of the Study Population.
IUGR - intrauterine growth retardation; APH- antepartum hemorrhage; PROM - prolonged rupture of membranes; CS - Cesarean section; RDS - respiratory distress syndrome. Table II Incidence and Severity of IVH (subgroup analysis).
*P = 0.03; IVH: intraventricular hemmorrhage; PVL: periventricular leukomalacia. On analysis of the data for secondary outcome measures, there was a significantly increased incidence of chronic lung disease (P = 0.005, RR 1.79, 95% CI 1.28-2.5) and bleeding episodes other than IVh (P = 0.04, RR 1.85, 95% CI 1.29-2.67) in the group that received indomethacin. On subgroup analysis for secondary outcome measures ( Table III), the bleeding episodes showed no significant difference between the indomethacin and the control in both the subgroup weight categories. However, the incidence of chronic lung disease continues to remain significantly higher ( P = 0.04) in the lower birth weight subgroup that received indomethacin and there was a significantly lower incidence of PDA in the higher birth weight subgroup (P = 0.02) respectively. The incidence of other secondary outcome measures was similar between indomethacin and controls amongst both the subgroups.Table III Incidence of Other Adverse Outcomes (subgroup analysis).
*P = 0.04; †P = 0.02; PDA: patent ductus arteriosus; NEC: necrotizing enterocolitis; CLD: chronic lung disease. The baby who developed renal failure received only one dose of indomethacin and died eventually despite peritoneal dialysis. Of those who were eligible for receiving indomethacin, 12 (9 in the first and 3 in the second weight category) could not complete the course after receiving the first dose because of the following reasons (a) Urine out put <0.5ml/kg/hr in 3; (b) High creatinine level in 2; (c) High potassium levels >7 mEq/L in 3; (d) Major IVH in 3 patients. Two subjects from the control group died within sixty hours of enrolment, the same time taken for receiving three doses of indomethacin as per protocol. These belonged to the lower birth weight category. On analysis of the data excluding these subjects, the incidence of major grade IVH was still significantly higher among the indomethacin group in the lower weight category and the significant differences noted for chronic lung disease persisted. These subjects were therefore included in the analysis on an intention to treat basis. Posthoc test estimated the power of the study to be 70% for this interim analysis. Discussion The present study was undertaken to test the efficacy and complications of indo-methacin prophylaxis in our population, which is entirely of Asian origin. To the best of our knowledge no data is currently available in the Asian population. We have experience with the use of indomethacin, since we have been using it for closure of PDA for several years now. Our data from the period before 1998 had shown a relatively high incidence of major grades of IVH. Hence it was appealing for us to embark on this trial. We were however disappointed with the results. Our results are contrary to the published data(6-9). Instead of seeing a reduction in the incidence of major grades of IVH, our data has shown that indomethacin prophylaxis made no difference. In fact, in the subgroup of babies with birth weight below 1000 g the incidence actually increased. There was also a significant increase in the incidence of chronic lung disease in the babies who received indo-methacin. Bleeding episodes other than IVh like gastrointestinal bleed, pulmonary hemorrhage and bleeding from puncture sites were also more in the treatment group. One case each of renal failure and PVL was also a matter of concern. There was no increase in the incidence of necrotizing interocolitis. The only benefit was an expected significant reduction in the incidence of symptomatic PDA. However, this effect was entirely confined to the higher birth weight sub- group. Bleeding is a potential complication due to the known effect of indomethacin on platelet aggregation. Norton, et al.(10) have shown an increase in the incidence of IVH following antenatal administration of indomethacin for prevention of preterm labor. Ours is probably the first study, which showed an increase in IVH rate with low dose indo-methacin prophylaxis postnatally. Although it has been suggested in literature that there is no need for ultrasound examination prior to indomethacin(11,12), the potential for extension of bleeding cannot be ignored. Renal failure and PVL are also expected complications of indomethacin. An increase in the incidence of chronic lung disease is surprising, though it has been reported in literature after the use of indomethacin antenatally to prevent pre- term labor(13). The likely explanation is the modulation of inflammatory mediators brought about by inhibition of cyclooxygenase by indomethacin, which results in increased availability of arachidonic acid for the formation of leukotrienes(14). Leukotrienes have been implicated in the pathology of chronic lung disease. Indomethacin exposure has also been shown to significantly decrease the alveolar volume and delay development of lamellar bodies in human and animal fetuses(15,16), another potential cause for lung damage. Volpe raised concerns about the possible adverse effects of indomethacin prophylaxis in a commentary in 1994(17). However, in the systematic review by Fowlie recently, it was shown that the prophylaxis is safe and concerns about adverse effects are largely unsubstantiated(18). This was based entirely on meta-analyses of studies from North America dealing with Caucasian or American African population. Sufficient data is lacking with regards to short-term and long-term complications in specific sub groups such as extreme low birth babies (<1000 g) and also in babies with different ethnic background. This is an interim mid-term analysis, the numbers are small to categorically dismiss the use of this potential prophylactic modality but we are concerned and would like to see more data from different ethnic populations and in babies below 1000 g. The fact that there was a decrease in the incidence of major grades of IVH in the control group without any specific intervention during the study period compared to our data before 1998 also raises doubts about the need for indomethacin prophylaxis in our setting. We have therefore discontinued the study. Contributors: PAKN conceived the design, involved in execution of the study and preparation of the manuscript; will be the guarantor of the study, MGP, HARG and DEDC were involved in the conduct of the study, interpretation of data and drafting the manuscript. SMAK assisted with conceiving the design of the study. Funding: None. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()