|
|
Case Reports Indian Pediatrics 2000;37: 667-670 |
|||||||||
|
Mediastinal Enteric Cyst Infected with Salmonella typhi |
|||||||||
|
Enteric cysts in posterior mediastinum are infrequently reported. They are mostly asymptomatic(1). We report a case of gastro-enteric cyst in posterior mediastinum infected with Salmonella typhi.
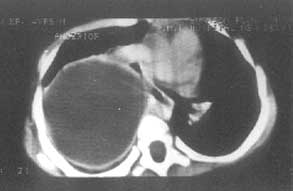
A 4½-year-old child was admitted with high grade intermittent fever and spasmodic paroxysmal cough of six days duration. He was a product of normal vaginal delivery, to non-consanguineous parents. There was past history of eight such episodes of fever and cough since infancy, the last episode being one month back. There was no history of cyanosis, hemoptysis, dyspnea on exertion, chest pain or rash. Examination revealed a febrile, toxic child with hepatosplenomegaly of 2 cm and 1 cm, respectively. His weight, height and head circumference were between 25th and 50th percentiles for age. The percussion note was dull and breath sounds were decreased on right side of chest posteriorly and in the axilla. Crepitations were heard bilaterally. Rest of the general physical and systemic examination was normal. Investigations revealed a polym-orphonuclear leukocytosis of 77% in a total leukocyte count of 14000 per cubic deciliter. Hemoglobin, blood urea, sugar, electrolytes and urine examination were normal. The skiagram of chest showed a right sided opacity in upper and mid zone (Fig. 1). The skiagram of thoracolumbar and cervical spine did not reveal any defects. Ultrasonography of chest revealed a cystic lesion in right upper chest. This was substantiated by contrast CT of chest, which showed a large well defined, smooth, homo-genous, right paratracheal cystic lesion with a regular enhancing wall, in the posterior and middle mediastinum, without any internal septation or calcification (Fig. 2). The cystic mass was displacing the right upper lobe bronchus anteriorly and compressing it. There was no significant lymphadenopathy. Mantoux test to 5 TU PPD did not evoke any reaction. ELISA for tuberculosis and IFA for Echinococcus were negative. Ultrasound guided fine needle aspiration was performed on right side of chest. The pus aspirated showed features of acute on chronic nonspecific abscess on light microscopy. On culture, Salmonella typhi was grown which was sensitive to cephalexin, cefotaxime, ceftriaxone, cipro-floxacin, ofloxacin, gentamycin and netilmycin and resistant to ampicillin, amoxicillin, chloramphenicol and cotrimoxazole. The patient was started on injection ciprofloxacin and cotrimoxazole. The patient was started on injection ciprofloxacin and gentamycin and a right posterolateral thoracotomy was per-formed. A thick walled infected cyst containing pus was seen in posterior mediastinum with pleural adhesions. These adhesions were removed and the cyst was dissected from the right side of posterior mediastinum. There was no communication of the cyst with esophageal lumen or any other viscera. Gross pathological examination revealed a gray brown unilocular cystic mass measuring 6 ´ 4 cm with dark brown shaggy inner surface. Cyst wall measured 0.5 cm. Microscopically the cyst was lined by gastric mucosa which was ulcerated at places and replaced by acute or chronic inflammatory granulation tissue. Cyst wall was bounded by double layer of smooth muscle and serosa. The repeat pus culture grew the same organism. The child was continued on same antibiotics for ten days. He had an uneventful post-operative period and was afebrile two days after surgery. He is doing well on follow up.
Posterior mediastinal cysts have been reported in about 7% of all posterior media-stinal masses in four series of 572 patients(1). Enteric cyst or enterogenous or esophageal cysts have been rarely reported. In two series reported they account for 0-4% of all posterior mediastinal masses(2,3). Enteric cysts may be located throughout posterior mediastinum or in neck. Most of them are asymptomatic at presentation, often discovered incidentally on skiagram of chest, taken for other indication(1). If they communicate with the lumen of respiratory tract, they may be symptomatic with respiratory features(1,4). Association with neural defects may be responsible for cord compression(5). Enteric cysts may be lined by esophageal or gastric epithelium surrounded by smooth muscle(1). They arise from the failure of coalescence of vacuoles early in the development of the foregut(1). To the best of our knowledge, there have been only two case reports of enterogenic cysts in mediastinum in children from India(5,6). Of these, one presented as paraplegia and the other was diagnosed incidentally. Our patient had high fever due to infected cyst. Salmonella typhi may have been seeded by the hematogenous route during the previous episode of pyrexia. Preoperatively it is difficult to distinguish the type of cyst. Radioisotopic study like Technetium 99 scan may be useful in diagnosis of enteric cyst. CT scan is a useful modality in defining the exact anatomic location of the cyst. The extent of involvement of vital structures also aids in determining the resectability(2). The exact type of cyst can only be known on histopathological examination. Excision of the cyst is the mainstay of treatment alongwith supportive care and antibiotic therapy if needed.
|
![]()