The novel
coronavirus (SAR-CoV-2) pandemic has disrupted
medical education worldwide [1]. Most of the medical
schools have quickly adapted to the online classes
with shifting of live clinical exposure with the
virtual one. Some schools also echoed concerns over
clinical clerkships and assessment during these
times. The COVID-19 pandemic represents a
transformation in medicine with the advancement of
telehealth, adaptive research protocols, and
clinical trials with flexible approaches to achieve
solutions [2-4]. We herein share our early initial
experience of online training of medical students in
the setting of COVID-19.
In wake of impending restrictions, we explored
available options for online classes and adopted G
Suite for Education using Google Classroom coupled
with Google Meet for Video-conferencing (https://edu.google.com/products/gsuite-for-education/?modal_active=none).
A schedule was made and messages were sent to
students by email and short messaging service (SMS)
to join their respective classes. An orientation
program was conducted to familiarize the faculty to
this platform. A team of trained faculty members was
deputed at the lecture venues to assist and
troubleshoot technical issues, if any. Additionally,
training videos were shared with faculty members.
In order to minimize excessive data usage by
students and preventing high screen time, a
four-hour teaching schedule, ensuring a judicious
mix of lectures and practical demonstrations/case
discussions were employed with a break of 10-15
minutes between sessions. To promote student
engagement, and to closely replicate laboratory and
clinical environment, short videos on lab procedure
and case based clinical examination were prepared
and shared on the virtual classroom. To make the
session interactive, students were encouraged to use
chat-box and switch on their microphones, wherever
feasible. Assignments were administered through
inbuilt plugins.
A questionnaire was prepared and administered via
Google forms to the students belonging to different
semesters of the MBBS course. The questionnaire was
reviewed and validated by the involved faculty
members. Participation was voluntary and complete
anonymity was ensured. Data was compiled using
spreadsheets. Gaussian fit of data was assessed
using Kolmogorov-Smirnov test.
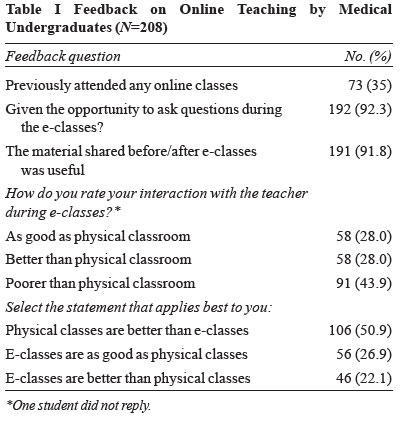
Across four batches from second to eighth semester,
398 medical undergraduate students were enrolled in
the classes; 208 provided their responses to the
questionnaire, with similar proportion across
various semesters (44-61%). The detailed responses
are depicted in Table I. The students,
based on their quantitative (Fig. 1)
and qualitative feedback, appreciated the online
platform. Large number of students had not attended
any online classes previously. Majority of the
students stated that they were given the opportunity
to ask questions (92.3%). They believed their
interaction with the teacher was better than (27%)
or as good as (27.8%) that during physical
classroom. The responses across semesters were also
uniformly similar.
 |
| |
| |
 |
|
Number of students in II, IV, VI and VIII
semesters was 61,47,44 and 56, respectively. |
Fig. 1
Rating of online classes during COVID-19
pandemic by medical graduates of different
semesters on a Likert scale of 1-10.
|
Interestingly, innovative solutions have emerged
whenever such problems have set in during SARS and
MRES outbreaks using telephone and virtual
environ-ment [5,6], and other adaptations during
COVID-19 [7]. While Moszkowicz, et al. [8]
implemented Google Hangouts for a similar purpose
but with only 10 students, we conducted concurrent
sessions for a large number belonging to four
different semesters. Our platform also supported
flipped classroom to some extent by providing
learning material in advance and promoting student
discussion during online sessions [9].
Student feedback revealed some interesting paradox.
While appreciative of the platform, nearly 50% of
the students still believed that physical classroom
was better than e-classroom. However, the reasons
for this perception could not be assessed. The study
was based on a small sample of students who have
anonymously volunteered to provide feedback.
Secondly, we had very short time to implement and
hence a well-structured training program for faculty
could not be done. This was; however, circumvented
to some extent, by the ease and self-explanatory
nature of the platform, a short explanatory video
and provision of technical support at lecture
venues. Furthermore, majority of our teachers got
adapted to this forum after taking a couple of
classes.
The novelty of the initiative lies in the swift
implementation of this program on a large scale both
for the students and for faculty members. Another
study from India has previously reported using the
same platform, but restricted to a single specialty
[10]. We believe our early experience can serve as a
model for educational institutes looking for
continuing medical education in situations that
disrupt traditional teaching.
Contributors:
All authors have contributed, designed and approved
the study.
Funding:
None; Competing interest: None stated.
REFERENCES
1.
Pather N, Blyth P, Chapman JA, Dayal MR,
Flack NAMS, Fogg QA, et al. Forced disruption
of anatomy education in Australia and New Zealand:
An acute response to the Covid-19 pandemic. Anat Sci
Educ. 2020 Apr 18. Available from
https://anatomypubs.onlinelibrary.
wiley.com/doi/epdf/10.1002/ase.1968. Accessed
April 23, 2020.
2.
Rose S. Medical student education in the time
of COVID-19. JAMA. 2020 Mar 31. Available from:
https://jamanetwork.com/journals/jama/fullarticle/2764138.
Accessed April 14, 2020.
3.
Liang ZC, Ooi SBS, Wang W. Pandemics and
their impact on medical training: Lessons from
Singapore. Acad Med. 2020 Apr 17. Available from
https://journals.lww.com/
academicmedicine/Abstract/9000/Pandemics_and_
Their_Impact_on_Medical_Training_.97208.aspx.
Accessed April 23, 2020.
4.
Li L, Xv Q, Yan J. COVID-19: The need for
continuous medical education and training. Lancet
Respir Med. 2020;8:e23.
5.
Patil NG, Yan YCH. SARS and its effect on
medical education in Hong Kong. Med Educ.
2003;37:1127-8.
6.
Park SW, Jang HW, Choe YH, Lee KS, Ahn YC,
Chung MJ, et al. Avoiding student infection
during a Middle East respiratory syndrome (MERS)
outbreak: A single medical school experience. Korean
J Med Educ. 2016;28:209-17.
7.
Hodgson JC, Hagan P. Medical education
adaptations during a pandemic: transitioning to
virtual student support. Med Educ. 2020 April 14.
https://onlinelibrary.wiley.com/doi/abs/10.1111/
medu.14177. Accessed April 23, 2020.
8.
Moszkowicz D, Duboc H, Dubertret C, Roux D,
Bretagnol F. Daily medical education for confined
students during COVID-19 pandemic: A simple
videoconference solution. Clin Anat. 2020 Apr 6.
Available from:
https://onlinelibrary.wiley.com/doi/full/10.1002/ca.23601.
Accessed April 23, 2020.
9.
Singh K, Mahajan R, Singh T, Gupta P. Flipped
classroom: A concept for engaging medical students
in learning. Indian Pediatr. 2018;55:507-12.
10.
Dash S. Google classroom as a learning
management system to teach biochemistry in a medical
school. Biochem Mol Biol Educ. 2019;47:404-7.


