The infection
rate of appendicitis may increase to up to 23% when perforation
occurs [1]. A 3-antibiotic regimen (cefmetazole, gentamycin, and
metronidazole) was in use in our hospital to decrease
postoperative infection. However, wound infection and
intra-abdominal abscess were noted in some cases of complicated
appendicitis (perforated or gangrenous appendicitis). We found
that 29% of our patients had a positive Pseudomonas sp.
culture of the appendix that was not covered by the above three
antibiotics. We switched our antibiotic regimen to piperacillin
and tazobactam and metronidazole, based on bacterial cultures
sensitivity tests of all complicated appendicitis cases in our
hospital. This new regimen, followed by oral ciprofloxacin, has
been in use in our department since April, 2013. Standardized
guidelines for patient care can help reduce infectious morbidity
[2]. We assumed that this protocol would decrease the infectious
complication rate. However, its net cost is higher than that of
the old protocol. Thus, we aimed to investigate the differences
in hospitalization duration and cost between the previous and
new antibiotic protocols.
This study was approved by the Research ethics review committee
of our hospital.
Charts of all patients (aged younger than 18 years (n=87)
who presented to our department from January, 2010 to August,
2016 with complicated appendicitis were reviewed
retrospectively. Laparoscopic appendectomy was performed with a
7-mm Jackson-Pratt drainage tube in all patients. A 3-antibiotic
regimen, followed by an oral antibiotic, was employed before
April, 2013, thereafter, pipiracillion- tazobactam and
metronidazole, and subsequent oral ciprofloxacin were used.
Patients were divided into two groups according to their
antibiotic regimen viz.
Group 1 patients received three antibiotics (cefmetazole
25 mg/kg 6-hourly, gentamycin 2.5 mg/kg 12-hourly, and
metronidazole 10 mg/kg 8-hourly). Group 2 patients received
piperacillin-tazobactam 112.5 mg/kg and metronidazole 10 mg/kg
8-hourly, followed by oral ciprofloxacin. Antibiotics were
administered intra-venously until patients were afebrile for
>24
hours and their appetite had recovered. All patients were
followed up in our outpatient department until full recovery.
Hospital costs in this study are estimates based on the current
pricing in our institution. The expense excluded the cost of
emergency room (ER) services and imaging studies performed in
the ER, and was calculated in United States dollars. Unpaired
2-tailed Student t-test and chi-square test were used to compare
data between both groups. P
<0.05
was considered significant. All analyses were performed using
SPSS version 20.0. (IBM Corp., Armonk, NY).
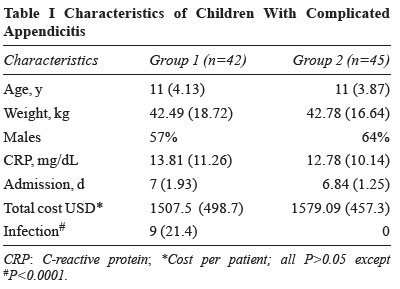
The patient demographics and
clinical outcomes are presented in Table I. The
durations of intravenous and oral antibiotics in group 2 were
3.95 and 5.8 days, respectively.
Nine patients in group 1 developed postoperative
complications, including 7 wound infections and 2
intra-abdominal abscesses (P<0.0001 when compared to
group 2). Three of these patients visited the ER because of a
wound infection or postoperative fever. The two patients with
intra-abdominal abscess were re-admitted. Therefore, the total
admission duration ranged from 4-16 (mean, 8.89) days. The total
cost increased significantly to $3613.34 (mean, $1824.00; P=0.03)
in patients with infectious complications compared to patients
who recovered uneventfully.
The study limitations were the
retrospective, single-centre design and small sample population.
Piperacillin-tazobactam has been recently demonstrated to
be as efficacious as traditional 3-antibiotic therapy [4,5].
The daily costs of receiving
intravenous antibiotics in our hospital in group 1 and 2 were
$18.27 and $88.73, respectively, for a child weighing 40 kg.
However, we found no difference in cost with the optimum
regimen, which is mainly related to the significant decrease in
infectious morbidity. Group 2 patients did not require further
antibiotic treatment and hospitalization. Generally, the cost of
managing infectious complications was significantly higher in
our study than in previous studies [6]. Therefore, we have
improved the quality of our medical care by the decreasing
infection rate without increasing cost.
It is important to use an effective
empirical antibiotic to control severe infection, but at the
same time, we should prevent antibiotic resistance. Therefore,
our principle is to monitor the duration of antibiotic use,
which can reduce the possibility of resistance [7]. Therefore,
piperacillin-tazobactan was not used for >7 days in our
patients.
We suggest that bacterial culture and sensitivity tests should
be performed for every case of complicated appendicitis, and
antibiotic protocol guided by these reports. Reducing
postoperative infectious morbidity in complicated appendicitis
using an optimum hospital-based antibiotic protocol can reduce
hospital stay without increasing expenses.
Contributors:
All authors were involved in patient care and manuscript
preparation, and are accountable for all aspects related to the
study.
Funding:
None; Competing interests: None stated.
REFERENCES
1. MacKellar A, Mackay AJ.
Wound and intraperitoneal infection following appendicectomy for
perforated or gangrenous appendicitis. Aust NZ J Surg.
1986;56:489-91.
2. Helmer KS, Robinson EK,
Lally KP, Vasquez JC, Kwong KL, Liu TH, et al.
Standardized patient care guidelines reduce infectious morbidity
in appendectomy patients. Am J Surg.
2002;183:608-13.
3. Lamb HM, Ormrod D, Scott
LJ, Figgitt DP. Ceftriaxone: An update of its use in the
management of community-acquired and nosocomial infections.
Drugs. 2002;62: 1041-89.
4. Paek H, Pham H,
Gagliardo C, Caruso-Prendergast P. Cefoxitin vs.
piperacillin/tazobactam for acute appendicitis in pediatric
patients. Open Forum Infect Dis.
2017;4:S500.
5. Youssif E, Aseeri M,
Khoshhal S. Retrospective evaluation of piperacillin–tazobactam,
imipenem–cilastatin and meropenem used on surgical floors at a
tertiary care hospital in Saudi Arabia. J Infect Public Health.
2018;11:486-90.
6. Capri S, Dellamano R.
Cost-effectiveness in the hospital use of antibiotics:
Introductory considerations. J Chemother. 1993;5:348-51.
7. Duration of antibiotic therapy and resistance. NPS
Medicinewise. National Prescribing Service Limited trading,
Australia. 13 June 2013.