Recently the
society of critical care medicine (SCCM) has published
evidence-based guideline of management of pediatric septic shock
and multi-organ dysfunction in children [1]. This guideline is
an update to the previously published version in the year 2017
[2] and the scope of guideline includes all term neonates (>37
wks) till end of childhood up to 18 year. Due to complex and
different pathophysiology of shock in preterms, the guideline
has not particularly looked for evidence pertaining to shock in
preterm neonates. In general, the words ‘suggested for’ or
‘suggested against’ have been used to denote ‘a weak
recommendation’ emerging from very ‘low to low-quality evidence’
for or against certain practice, respectively; while the words
‘recommended for’ or ‘recommended against’ have been used to
denote ‘strong recommendation’ for or against certain practice
arising from ‘moderate to high quality evidence’. However, some
of the recommendations in all the above mentioned categories
have also emerged as best practice statement, based on the
consensus opinion of experts when adequate evidence is not
available.
KEY CHANGES
As compared to previously published guideline the current
guideline is more extensive and detailed which covers supportive
and ancillary management of pediatric septic shock which were
henceforth not covered in the previous version. These include
details of evidence-based recommendation on antimicrobial
therapy, source control of infection, nutrition, ventilation,
prophylaxis against bedsore, deep vein thrombosis and ulcer. As
compared to previous guidelines, the current guideline has
de-emphasized the role of lactate in hemodynamic monitoring.
Similarly, it promotes restrictive fluid up to 40 mL/kg
(previously up to 60 mL/kg) and each bolus of 10-20 mL/kg
(previously 20 mL/kg) during resuscitation in settings where
there is no support of intensive care facility to avoid fluid
overload. As is the case in many health care facilities in
lower-middle income countries, where prevalence of malnutrition
in children is very high, unsupervised administration of high
volume of fluid can actually increase mortality. Hence the
current guideline has been more conservative in these scenario.
Further, it has set a time frame of 3 hour for initiation of
antibiotics in children with sepsis but without septic shock. In
light of recent emerging evidence the guideline has replaced
epinephrine or nor-epinephrine in place of dopamine as first
choice inotrope. However, its applicability in resource-limited
setting may remain an issue where these two drugs are not easily
available and dopamine may have to be used as first line drug in
these situations. As the recent guideline has not mentioned
exact cut-off of blood pressure for hypotension, normal range of
blood glucose or hemoglobin level cutoff for transfusion in
unstable children, for point of care issues related to these
topics, the readers still have to either refer the previous
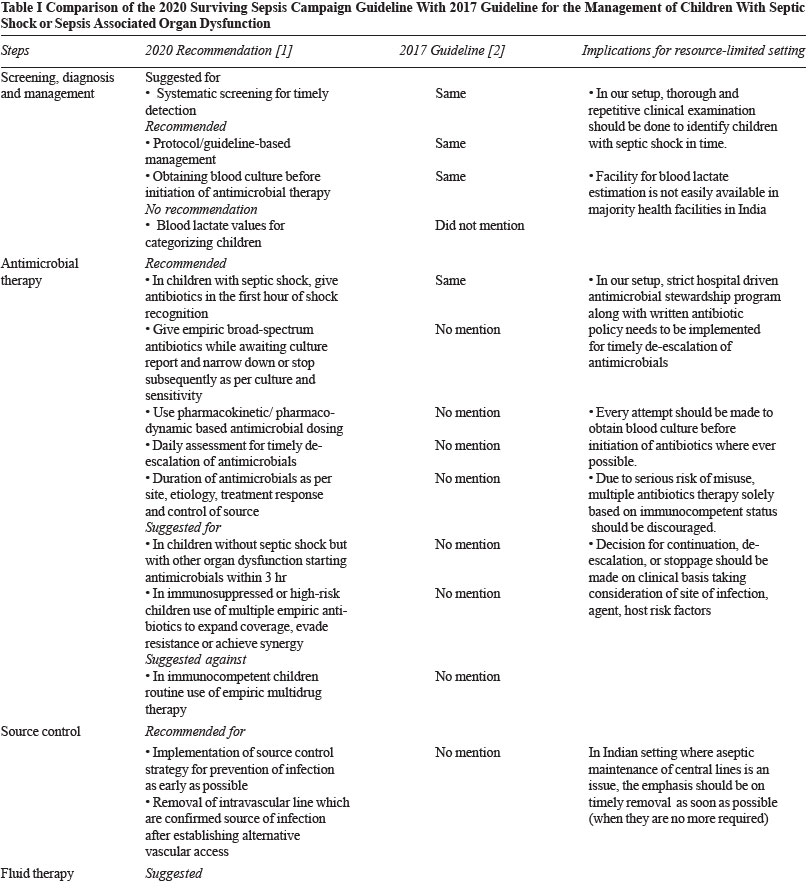
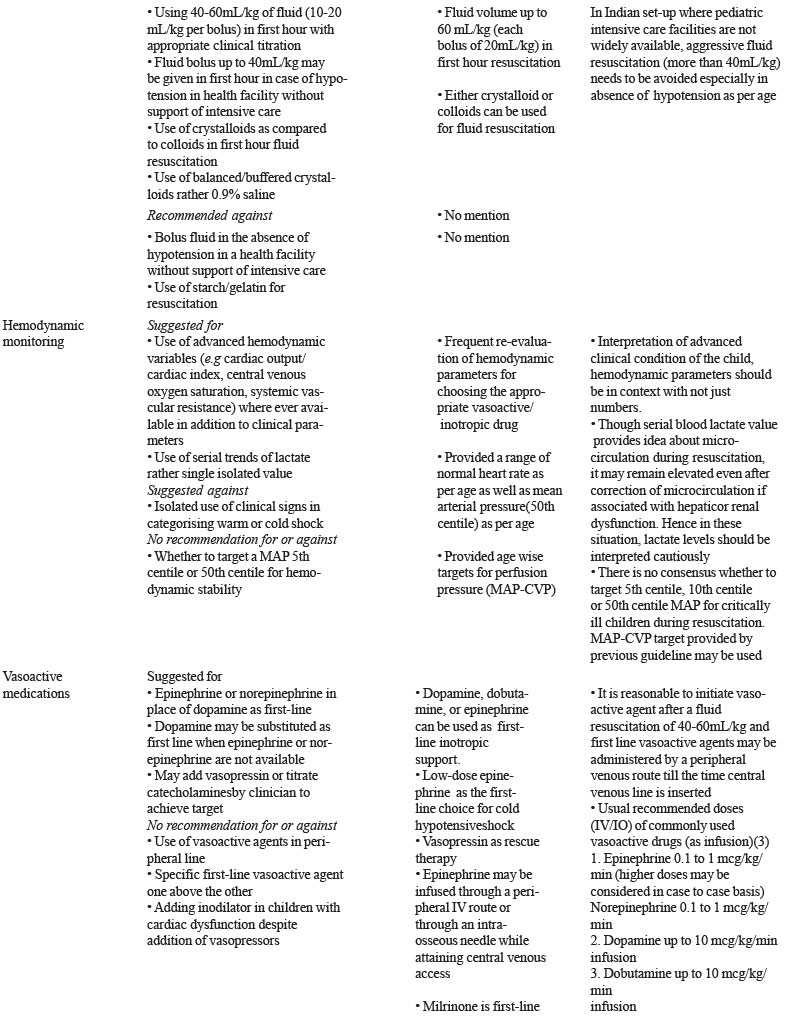
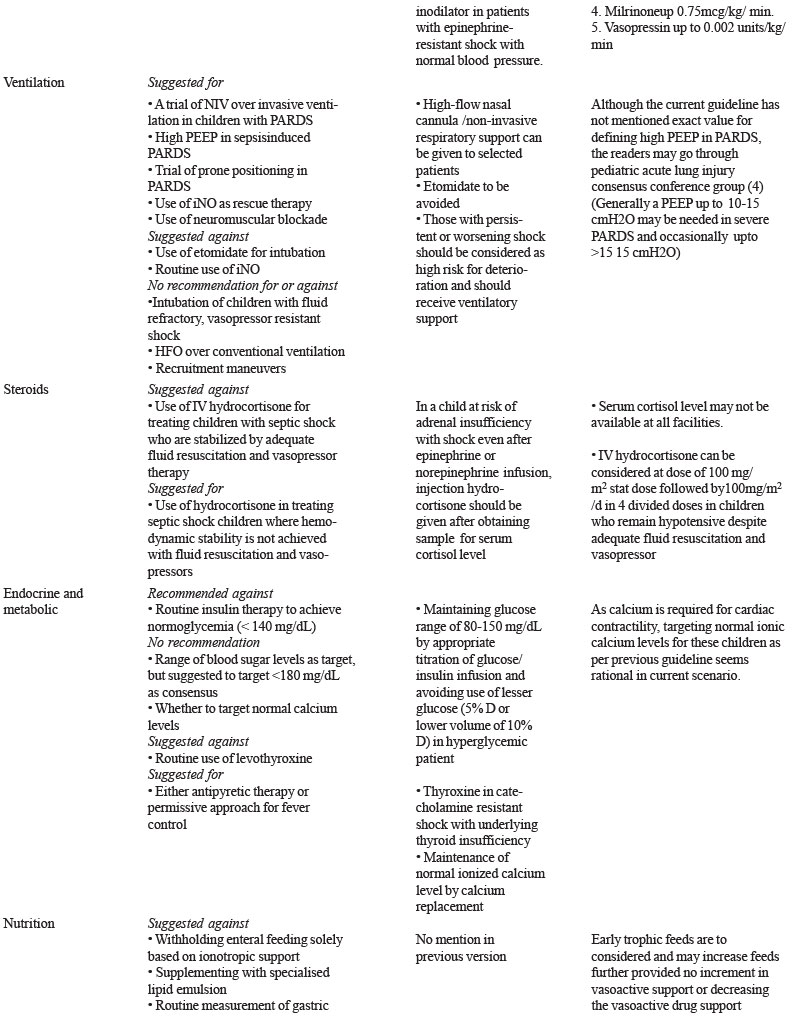
version or other published guideline. The summary of 2020
surviving sepsis campaign guideline in contrast with 2017
guideline has been provided in Table I.
THE WAY FORWARD
The current version
addressed practical issues pertaining to pediatric septic shock
management, which can be applicable to resource-limited setting
as well. Supportive aspects in management of septic shock such
as ventilation, antibiotic stewardship, and nutrition are
addressed compared to previous guidelines that concentrated more
on first hour management. Like with any other International
guidelines, the current guideline also needs to be adapted to
local clinical practice cautiously in the light of experience,
clinical acumen and judgment for its maximum
benefit/utilization.
Contributors:
TS, AS: both equally contributed in collection of literature and
drafted the manuscript; KMG: provided critical inputs in the
manuscript. All authors approved the final version.
Funding:
None; Competing interest: None stated.
REFERENCES
1. Weiss SL, Peters MJ, Alhazzani W, Agus MS, Flori HR, Inwald
DP, et al. Surviving Sepsis Campaign International
Guidelines for the Management of Septic Shock and
Sepsis-associated Organ Dysfunction in Children. Intensive Care
Med. 2020;46:10-67.
2. Davis AL, Carcillo JA, Aneja RK, Deymann AJ, Lin JC, Nguyen
TC, et al. American College of Critical Care Medicine
Clinical Practice Parameters for Hemodynamic Support of
Pediatric and Neonatal Septic Shock. Crit Care Med.
2017;45:1061-93.
3. American Academy of Pediatrics. Pediatric Advanced Life
Support (PALS) Provider Manual. American Heart Association;
2015.
4. Pediatric Acute Lung Injury Consensus Conference Group.
Pediatric Acute Respiratory Distress Syndrome: Consensus
Recommendations from the Pediatric Acute Lung Injury Consensus
Conference. Pediatr Crit Care Med. 2015;16:428-39.